

In the surgical treatjment of aesthetic midface concerns there are two different approaches, maxillary advancement or implant augmentation. While on the suface they may be seen as interchangeable they are quite different in their aesthetic effects and their indications. The following provides a detailed comparison betwen these differenves
How Is A Custom Midface Mask Implant Different Than A LeFort I Osteotomy?
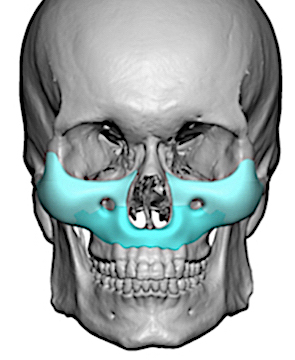
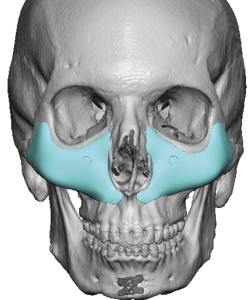
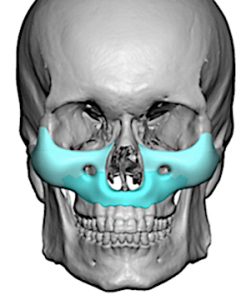 Custom Midface Mask implant
Custom Midface Mask implant
- Adds volume on top of the bone (infraorbital rim + malar + paranasal/maxilla) to simulate skeletal advancement.
- Best at changing surface contour: under-eye support, tear trough, cheek/paranasal fullness, midface convexity.
- Does not change dental occlusion or airway.
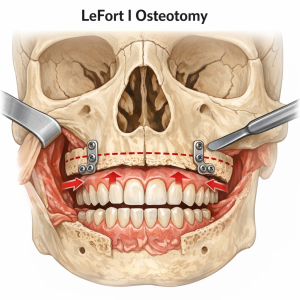
 Le Fort (usually Le Fort I; sometimes II/III in syndromic/trauma cases)
Le Fort (usually Le Fort I; sometimes II/III in syndromic/trauma cases)
- Moves the bone itself (maxilla ± infraorbital/zygoma depending on level).
- Best at changing skeletal position: bite/occlusion, maxillary projection, nasal base relationship, sometimes airway.
- Changes both hard tissue position and soft tissue drape more globally.
Aesthetic Effects
Under-eyes / infraorbital rim
 Mask implant: often excellent if the deficiency is rim/infraorbital + anterior maxilla; can “build a rim.”
Mask implant: often excellent if the deficiency is rim/infraorbital + anterior maxilla; can “build a rim.”- Le Fort I: has not effect of undereye area as the osteotomy level is much lower. May make a normal infrarbital rim projection look deficient or make a pre-existing deficiency greater. Only a Le Fort II/III addresses orbit/upper midface but is rarely used as an aesthetic or jaw repositioning procedure
 Mask implant: often excellent if the deficiency is rim/infraorbital + anterior maxilla; can
Mask implant: often excellent if the deficiency is rim/infraorbital + anterior maxilla; can Bottom line: for true infraorbital rim deficiency, an implant targets it directly, a Le Fort I not at all.
Cheeks & Paranasal region
- Mask implant: very controllable malar augmentation/shaping—paranasal fill, smooth transitions.
- Le Fort I: moves maxilla forward; paranasal support will improve, but cheek/zygoma changes will not occur as the osteotomy level is way below it.
 Le Fort I: moves maxilla forward; paranasal support will improve, but cheek/zygoma changes will not occur as the osteotomy level is way below it.
Le Fort I: moves maxilla forward; paranasal support will improve, but cheek/zygoma changes will not occur as the osteotomy level is way below it.Nasolabial folds / upper lip support
- Le Fort I: stronger effect when upper lip support is skeletal/occlusal-driven.
- Mask implant: can help via paranasal/anterior maxillary augmentation, but will have not have any effect on upper lip support.
Nose changes
- Le Fort I: commonly affects nasal base/upper lip dynamics (alar width, nasal tip rotation can change), often needs alar cinch and V-Y closure considerations.
- Mask implant: can have an indirect nasal base change (nostril widening), may ned an alar base cinch suture to prevent
Functional effects (big divider)
Bite / occlusion
- Le Fort: can correct malocclusion (Class III, open bite, etc.). This is the main reason to do it.
- Mask implant: cannot fix occlusion.
Airway / speech / chewing mechanics
- Le Fort: can improve all three functions in select cases, the significant of these benefits is usually related to the degree of forward advancement.
- Mask implant: cosmetic effect only, no functional benefits
Predictability and Precision
- Mask implant: high aesthetic precision (CAD control over mm-level contour and symmetry). Great for asymmetry and targeted deficiency.
- Le Fort: very powerful but depends on surgical planning, orthodontics, relapse control; still predictable in good hands, but outcomes are more “movement-driven” than “sculpting-driven.”
Surgery and Recovery
Mask implant
- Surgery is localized but still significant dissection.
- Typical risks: infection, malposition, palpable edge, lower lid issues if infraorbital approach, sensory changes.
- Recovery: swelling can be significant; tends to be simpler than orthognathic surgery overall.
Le Fort advancement
- Bigger operation: hospital/OR time, fixation, sometimes orthodontics.
- Risks: bleeding, infection, numbness, sinus/nasal issues, relapse, dental/occlusal changes, need for orthodontic coordination.
- Recovery: generally more intense and longer.
Reversibility / Revision
- Mask implant: removable/replaceable (still not trivial, but conceptually reversible).
- Le Fort: not “reversible” in the same way; revisions are possible but more involved.
When each is usually the better choice
Mask implant tends to win when:
- Occlusion is acceptable (or patient doesn’t want orthognathic).
- Primary goal is under-eye/infraorbital support + paranasal + cheek contour.
- There’s asymmetry needing custom correction.
- You want sculpting control rather than broad skeletal movement.
Le Fort tends to win when:
- There’s a bite problem or functional indication.
- The aesthetic issue is mainly maxillary position (retrusion) rather than contour.
- Patient is prepared for orthodontics/recovery and wants a “true skeletal move.”
- Obstructive sleep apnea needs to be improved
Practical “decision shortcut”
- If the bite is wrong ? Le Fort.
- If the bite is fine and the midface looks flat/deflated—especially under the eyes ? custom mask implant (often + soft-tissue work).
- If both are issues: Le Fort first, then consider secondary contouring (implants/fat) if needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon