


Soft-tissue jaw angle implants can be a very useful solution for masseteric muscle dehiscence, but only in select scenarios and with the right implant design and surgical strategy.
The Problem: Masseteric Muscle Dehiscence
Masseter muscle dehiscence typically presents as:
- Soft tissue posteroinferior hollowing at the mandibular angle
- Can make the bony or implanted jaw angle look skeletonized
- Almost always iatrogenic (prior or existing angle implants)
- Sometimes associated with animation deformity, the hollow becomes more prominent when clenching or chewing as it lacks muscle.
Bone-based angle implants can not correct a soft tissue contour deformity. In fact it will magnify it. This is because the deficiency is soft tissue, not skeletal in origin.
Role of Soft Tissue Jaw Angle Implants
Indications
Soft tissue angle implants are most effective when:
- The mandible itself has adequate bony width
- The deformity is due to muscle detachment, thinning, or atrophy
- There is a static hollow which is exaggerated by dynamic animation
- Can be used whether there is an underlying jaw angle implant or not
Implant Design Considerations
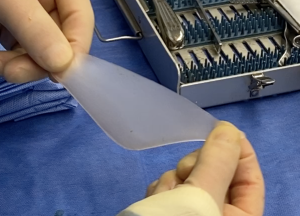
Material
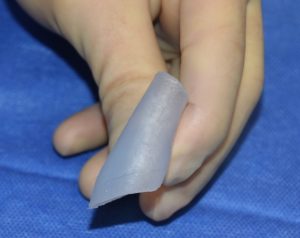
 Silicone remains the only practical material to use as it must match the consistency/feel of muscle or soft tissue
Silicone remains the only practical material to use as it must match the consistency/feel of muscle or soft tissue- A low durometer silicone material is used just like that in temporal muscle implants
 Silicone remains the only practical material to use as it must match the consistency/feel of muscle or soft tissue
Silicone remains the only practical material to use as it must match the consistency/feel of muscle or soft tissueShape
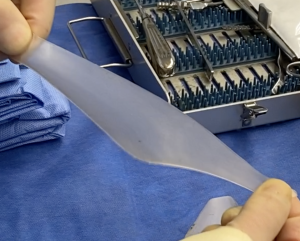
- Isosceles triangle shape with horizontal axis longer than the vertical for posterolateral jaw angle shape
- The exact implant dimensions used are from measurements of the soft tissue contour deficiency which if bilateral are rarely symmetric
 Isosceles triangle shape with horizontal axis longer than the vertical for posterolateral jaw angle shape
Isosceles triangle shape with horizontal axis longer than the vertical for posterolateral jaw angle shape T
T he exact implant dimensions used are from measurements of the soft tissue contour deficiency which if bilateral are rarely symmetric
he exact implant dimensions used are from measurements of the soft tissue contour deficiency which if bilateral are rarely symmetricThickness
- The greatest implant thickness is at the ‘gonial angle’ area of the implant, usually 5 to 7 mms
- The implant thickness tapers from the angle out to the anterior superior and posterior implant edges where it goes down to feathered edges
Surgical Plane & Technique
Incision and Plane
- Transcutaneous approach with direct curved incision at back of bony jaw angle, 10 to 15mms in length
- Direct dissection down to fascia or deep subcutaneous plane, not subfascial, submasseteric or subperiosteal
- Goal: replace lost muscle bulk, not displace remaining fibers

 Transcutaneous approach with direct curved incision at back of bony jaw angle, 10 to 15mms in length
Transcutaneous approach with direct curved incision at back of bony jaw angle, 10 to 15mms in lengthImplant Placement and Fixation
- Precise pocket creation that is no bigger than the implant but in which the implant lies passively with no folds or bends
- Stability of implant position in soft tissue is pocket control
- Holes can be placed in the implant to allow for through and through soft tissur ingrowth
- In some cases it may possible to secure it to an underlying implant if present with a screw…keeping a soft tissue layer between them
 Holes can be placed in the implant to allow for through and through soft tissur ingrowth
Holes can be placed in the implant to allow for through and through soft tissur ingrowthWhat Soft Tissue Implants Do Well
– Restore angle shape
– Mask muscle detachment
– Improve symmetry
– Avoids intraoral approach, reduces risk of infection, ease of recovery with minimal swelling and no adverse effect on mouth opening and chewing
What They Do NOT Do
- ?Reattach muscle
- ?Provide any functional benefit
- ?Decreases but may not eliminate severe animation deformity
Non-Implant Graft Alternatives
- Autologous dermal-fat grafts (unpredictable volume retention, contour irregularities)
- Alloderm / ADM (inadequate volume/thickness)
- Injection Fat Grafting the one option most commonly tried first by many surgeons and to which soft tissues implants should be compared in terms of aesthetic outcomes, longevity, behavior with animation, ease of revision and best indications for its use.
Soft-Tissue Jaw Angle Implants (Silicone)
Aesthetic Outcome
- Most predictable correction of posteroinferior hollowing
- Restores angle continuity and vertical length
- Excellent static symmetry
- Good camouflage even with partial muscle loss
Longevity
- Permanent
- No resorption
- Stable in scarred tissue beds
Behavior With Animation
- Masks deformity at rest
- Does not worsen animation
- Mild animation deformity may persist but is less visible
Revision Friendliness
- Easily removable or modifiable
- Minimal additional muscle trauma
Best Use Case
- True masseteric muscle dehiscence
- Prior angle implant complications
- Patients who want a one-and-done solution
Fat Grafting by Injection
Aesthetic Outcome
- Can soften very mild hollows
- Poor recreation of angle geometry
- Creates fullness not definition
Longevity
- Unpredictable resorption (30–70%)
- Often requires multiple sessions
Behavior With Animation
- Fat stays static in position while masseter muscle expands
in movement - Hollow may paradoxically look deeper on clenching
Revision Friendliness
- Repeated grafting does not makes later implant placement more difficult
Side-by-Side Summary
|
Feature |
Soft Tissue Implant |
Fat Grafting |
|
|
Predictability |
????? |
?? |
|
|
Longevity |
Permanent |
Variable |
|
|
Angle Definition |
Excellent |
Poor |
|
|
Animation Risk |
Low |
Moderate |
|
|
Revision Safety |
High |
Moderate |
|
|
Ideal for Dehiscence |
Yes |
No |
Clinical Takeaway
For masseteric muscle dehiscence:
- Soft-tissue jaw angle implants are the best balance of predictability, safety, and aesthetics.
- Fat grafting alone is rarely sufficient and often disappointing long-term.
Practical Strategy That Works Well
Fat injections or synthetic fillers is often done first as it is the most appealing to many patients particularly if the soft tissue contour deficiency is modest
Soft-tissue angle implants should be first strategy for more significant contour deformities or more modest ones that have failed initial injection strategies
Bottom Line
For masseteric muscle dehiscence, soft tissue jaw angle implants are often the best structural camouflage option. The key is designing the implant to replace the missing muscle, not bone.
Dr. Barry Eppley
Plastic Surgeon