

Posterior webbed neck correction is a posterior midline excisional technique used to improve the contour of a webbed neck. It is an indirect surgical approach that emphasizes scar concealment.
Rather than directly excising or rearranging the lateral neck webs—which produces visible scars along the sides of the neck—the posterior approach moves the webs inward through a midline posterior tissue pull.
Concept Overview
The deformity in a true webbed neck typically consists of:
- Lateral skin excess (horizontal redundancy)
- Deep trapezial fascial banding
- A blunted cervico-shoulder angle
- A low posterior hairline
The posterior approach corrects these issues by:
- Removing a central wedge of excess skin and fat on the back of the neck
- Releasing deep fascial bands
- Performing midline fascial and muscle plication
- Pulling lateral neck tissues medially
In essence, the procedure converts horizontal tissue excess into a vertical closure.
Case Study
An adult female with moderate, non-syndromic neck webbing presented for surgical improvement.
Key Surgical Steps
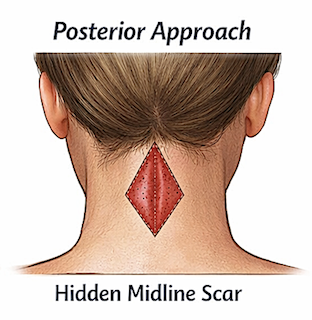
Incision Design

 Diamond (Midline Wedge) Pattern
Diamond (Midline Wedge) Pattern
- Placed in the posterior midline
- Half of the excision lies within the occipital hairline
- The remaining half lies in the posterior neck skin
- The width of the diamond is determined by the pinch test
 Skin Excision
Skin Excision
- Full-thickness excision of skin and fat down to the muscle fascia
- The excision must be large enough to create a strong medial pull on the lateral neck tissues
- Undercorrection of the diamond excision increases the risk of recurrence
Fascial Release
This is a critical step in the procedure.
Key components include:
- Release of trapezial fascial bands
- Freeing lateral tethering
- Midline fascial plication
- Allowing significant medial redraping of neck tissues
Failure to adequately release these structures is the most common cause of recurrence.
 Contour Reapproximation
Contour Reapproximation
- Deep sutures are placed to reshape the trapezial contour
- Tension is redistributed centrally
- This reduces tension on the skin closure

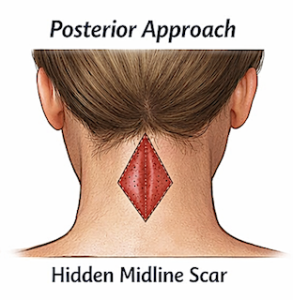
 Her immdeiate results shopwed visible reduction of her neckl webs.
Her immdeiate results shopwed visible reduction of her neckl webs.

 The posterior approach leaves half of the scar up in the hair and the other half down the backj of the neck skin.
The posterior approach leaves half of the scar up in the hair and the other half down the backj of the neck skin.
Advantages
- Strong medial correction vector
- Effective for mild to severe neck webs
- Lower recurrence rates compared to skin-only lateral techniques
- Provides direct structural reshaping
Trade-Offs
- Vertical posterior midline scar
- Potential scar widening in high-tension closures
- Does not directly improve anterior neck aesthetics (e.g., submental fullness)
- Risk of hypertrophic scarring in some patients
- Some secondary relaxation may occur over time and may require minor scar revision
- Webbing is reduced but not always completely eliminated
Practical Summary
Posterior webbed neck correction is a reconstructive contour procedure that:
- Removes horizontal skin excess
- Releases deep structural bands
- Recreates a more normal cervico-shoulder angle
- Trades a vertical posterior scar for improved and more durable contour
Discussion
Complete elimination of neck webbing does not occur in the majority of patients. Realistic surgical goals include:
- Significant contour improvement
- An acceptable scar trade-off
- Long-term structural stability
For this reason, webbed neck surgery should be viewed not as complete correction but as reduction in the appearance of the webs.
 The posterior approach treats the deformity from a remote or indirect location. Instead of directly excising the webs, it reduces their prominence by relocating and tightening surrounding tissues.
The posterior approach treats the deformity from a remote or indirect location. Instead of directly excising the webs, it reduces their prominence by relocating and tightening surrounding tissues.
Because the webs are repositioned rather than removed, some degree of recurrence or relapse—defined as partial re-formation of lateral webbing—can occur. This depends on:
- Surgical technique
- Severity of the deformity
- Tissue characteristics
What “Recurrence” Actually Means
Recurrence may present as:
- Gradual return of lateral skin webbing
- Blunting of the neck-shoulder angle
- Scar widening, which may mimic persistent webbing
In most cases, any recurrence becomes apparent within 6 to 8 weeks after surgery.
Revision Surgery
A secondary or revision procedure may be considered if:
- Persistent lateral bands remain
- Contour correction is inadequate
- Asymmetry develops
Revision procedures are typically more limited and targeted.
In Practical Terms
The risk of recurrence primarily depends on:
- Severity of the original deformity
- Whether deep fascial bands were adequately released
- The surgical correction vector
- Patient age
- Tissue characteristics
When structural correction is properly performed, long-term stability is generally good, although this is not a zero-recurrence operation.
Dr. Barry Eppley
Plastic Surgeon