

A brow bone reduction can be reversed with a custom brow bone implant in selected patients. The usual concept is to use a patient-specific implant designed from a current 3D CT scan to rebuild projection of the supraorbital ridge/brow area. That is a recognized approach in facial masculinization, where forehead/brow augmentation may be done with implants or other augmentative materials.
The main issue is not whether an implant can be made, but whether the anatomy is favorable after the prior reduction. A current 3D CT scan is important to check how the prior brow reduction healed, especially if a frontal sinus setback/bone flap was done. The key concern is whether there has been solid bony healing and whether elevating the soft tissue over the area would risk entering or exposing the frontal sinus.
A few practical points:
- Best candidate: someone who had prior brow bone reduction/forehead feminization and now wants more brow projection restored.
- Planning: a new CT-based custom implant is typically used because off-the-shelf brow bone implants do not exist.
- Expected result: the implant can restore bony projection, but it may not reliably reposition the eyebrow hairs/arch the way patients hope; eyebrow soft tissue response is less predictable than bone contour change.
- Access/scarring: prior hairline/scalp incisions can sometimes actually be useful for access, depending on how the original surgery was done.
The main limitations and risks are the same ones you would want discussed in detail before surgery: infection, implant malposition/asymmetry, palpability/visibility if thin soft tissue, contour irregularity, need for revision, numbness, and frontal sinus-related issues if the prior reduction involved the sinus. The sinus anatomy and bone healing status are what make the CT scan so important.
So the bottom line is: technically feasible, often best done with a custom implant, and the deciding factor is the current CT anatomy after the original reduction.
Case Study
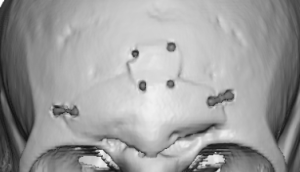
 This male had facial feminization surgery previously but decoded to reverse that decision and re-masculinize his face. A 3D CT scan showed a well healed bone flap n around most of its edge with multiple sites of hardware fixation. On the bottom side of the bone flap there was some non-bony healed gaps along the frontonasal junction.
This male had facial feminization surgery previously but decoded to reverse that decision and re-masculinize his face. A 3D CT scan showed a well healed bone flap n around most of its edge with multiple sites of hardware fixation. On the bottom side of the bone flap there was some non-bony healed gaps along the frontonasal junction.
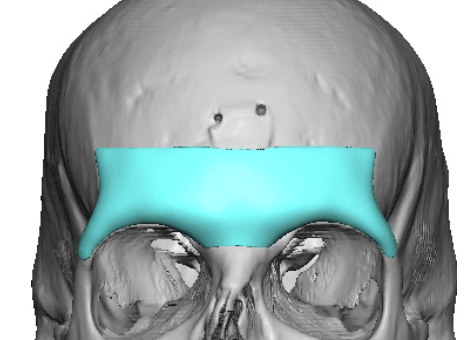
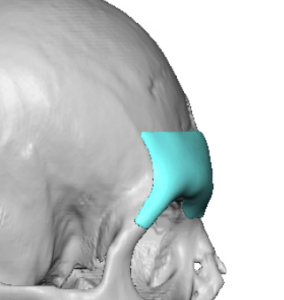 A custom brow bone implant was designed with a total volume of 7ccs which covered most of the healed bone flap.
A custom brow bone implant was designed with a total volume of 7ccs which covered most of the healed bone flap.
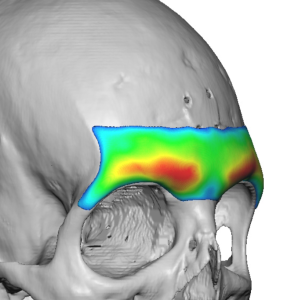 The distribution of the implant’s thicknesses was the greatest over the medial brow area.
The distribution of the implant’s thicknesses was the greatest over the medial brow area.

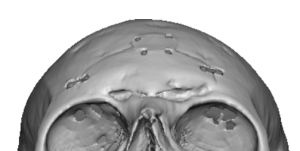
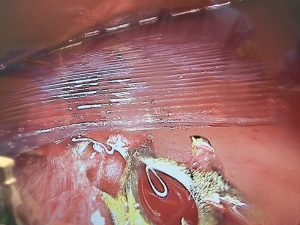 The implant was placed through a small incision just behind the central frontal hairline with endoscopic visual assistance.The fixation hardware could be visualized but was no a hindrance to the implant/s placement.
The implant was placed through a small incision just behind the central frontal hairline with endoscopic visual assistance.The fixation hardware could be visualized but was no a hindrance to the implant/s placement.
T he implant was secured with a small micro screw at its tailpipe over the upper lateral orbital rim through a small eyelid incision.
he implant was secured with a small micro screw at its tailpipe over the upper lateral orbital rim through a small eyelid incision.

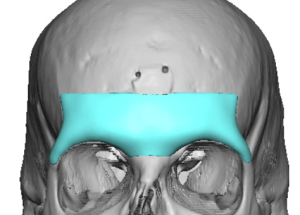
 The brow bone augmentation effect was immediately apparent.
The brow bone augmentation effect was immediately apparent.
Discussion
The CT scan is really the “decision-maker” for how easy—or risky—a brow bone implant reconstruction will be. What you’re looking at is how the prior reduction altered the frontal bone and sinus, and how much stable structure remains to build on.
? Findings that make reversal more straightforward
These cases are usually very favorable for a custom implant:
1. Intact or minimally altered frontal sinus
- Outer table reduced (burring) but no osteotomy/bone flap
- Sinus cavity remains undisturbed
? This is ideal because: - Solid bone surface for implant fixation
- Lower risk of sinus-related complications
2. Good bony thickness of the supraorbital rim
- Residual bone ? a few millimeters across brow ridge
- No areas of extreme thinning or translucency
? Allows: - Stable implant seating
- Lower risk of contour irregularities or palpability
3. Smooth, continuous forehead contour
- No step-offs, gaps, or irregular healing
- Symmetric reduction pattern
? Makes implant design easier and more predictable
4. No hardware or well-positioned hardware
- Either no plates/screws, or they are flush and not interfering
? Avoids: - Need for removal or redesign complications
5. No sinus violation or scarring into soft tissue plane
- Clean separation between bone and overlying soft tissue
? Easier dissection and lower infection risk
? Moderately complex findings
These cases are still doable, but require more careful planning:
1. Prior frontal sinus setback (bone flap)
- Evidence of:
- Osteotomy lines
- Repositioned anterior table
- Bone flap appears healed and stable
? Implications: - Implant can still be done
- Must avoid disrupting the sinus or flap
2. Patchy bone thinning
- Areas of very thin outer table
- Especially over sinus
? Risks: - Palpability/visibility of implant edges
- May require softer transitions or thicker implant design
3. Mild contour irregularities
- Small step-offs or asymmetries
? Requires: - More complex custom implant design to camouflage
4. Existing fixation hardware
- Plates/screws from prior setback
? Options: - Leave in place and design around them
- Or remove during surgery (adds complexity)
? More complex / higher-risk findings
These are the situations where reversal becomes technically demanding:
1. Extensive frontal sinus violation or irregularity
- Irregular sinus contour
- Partial resorption or remodeling of anterior table
- Possible communication with soft tissue
? Concerns: - Infection risk
- Implant positioning over unstable sinus wall
2. Very thin or deficient bone
- Outer table extremely thin or absent in areas
? Problems: - Poor implant support
- Higher risk of contour show-through or complications
3. Non-union or unstable bone flap
- Incomplete healing of prior setback
- Visible gaps or mobility (rare but important)
? May require: - Bone repair before or along with implant
4. Significant asymmetry or irregular reconstruction
- Uneven prior reduction
- Distorted anatomy
? Requires: - Highly customized implant
- More artistic than purely structural reconstruction
5. Sinus obliteration or unusual anatomy
- Sinus filled, scarred, or surgically altered
? Makes: - Dissection and implant placement less predictable
? What the surgeon is really assessing
From a planning standpoint, the CT answers three critical questions:
1. Is there a stable foundation?
- Solid bone vs thin/irregular surface
2. Is the frontal sinus safe?
- Intact vs altered vs risky to re-enter
3. Can a custom implant sit predictably?
- Smooth surface vs distorted anatomy
? Bottom line
- Simple reduction (burring only) ? usually very straightforward reversal
- Well-healed sinus setback ? doable but more technical
- Irregular, thin, or unstable anatomy ? complex and higher risk
Dr. Barry Eppley
Plastic Surgeon