

 Ideal candidate selection for custom midface mask implants is less about “wanting more cheek volume” and more about having a true structural midface deficiency that benefits from unified skeletal augmentation.
Ideal candidate selection for custom midface mask implants is less about “wanting more cheek volume” and more about having a true structural midface deficiency that benefits from unified skeletal augmentation.
Good Candidates (Who benefits most)
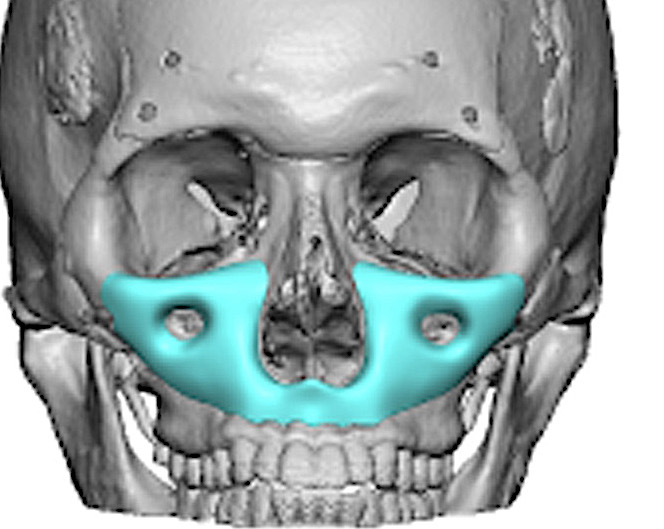
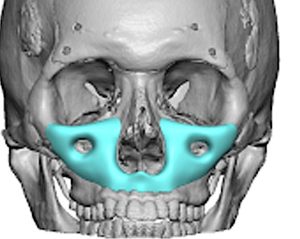
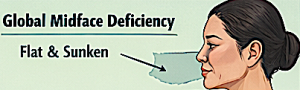
1. Global midface deficiency (key indication)
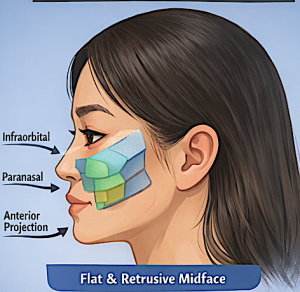
 Flat or retrusive midface when viewed from profile
Flat or retrusive midface when viewed from profile- Poor anterior projection of:
- Infraorbital rim
- Maxilla
- Paranasal region
- Often described as a “sunken” or “concave” midface
 Flat or retrusive midface when viewed from profile
Flat or retrusive midface when viewed from profileThese patients benefit most because the implant restores forward projection as a unit, not just spot volume.
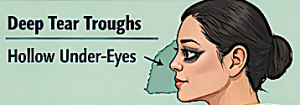
2. Prominent tear troughs due to bone deficiency
- Deep tear troughs that:
- Don’t respond well to fillers
- Recur quickly after treatment
- Caused by lack of infraorbital support (not just soft tissue)
 Deep tear troughs that:
Deep tear troughs that:
Midface implants address the underlying skeletal problem, not just camouflage it.
3. Flat paranasal region
- Weak support around the base of the nose
- Deep nasolabial folds from skeletal deficiency (not aging alone)
 Weak support around the base of the nose
Weak support around the base of the noseEspecially relevant in many Asian patients where paranasal retrusion is common.
4. Patients who look “tired” despite good skin quality
- Hollow under-eyes
- Lack of light reflection in midface
- Disproportion between lower eyelid and cheek
This is often structural—not a skin or aging issue.
5. Failed or insufficient prior treatments
- Fillers requiring frequent maintenance
- Fat grafting with poor retention
- Standard cheek implants that look:
- Too lateral
- Disconnected from infraorbital region
 Fillers requiring frequent maintenance
Fillers requiring frequent maintenanceCustom implants provide a more continuous, anatomical correction.
6. Desire for permanent, structural change
- Patient understands:
- This is not subtle like filler
- Results are long-lasting and not easily reversible (especially with Medpor/PEEK)
Borderline Candidates (Proceed cautiously)
1. Primarily soft tissue aging (not skeletal deficiency)
- Mild tear troughs
- Good bone structure but:
- Skin laxity
- Fat descent
 Good bone structure but:
Good bone structure but:
? Better treated with:
- Lower blepharoplasty
- Fat repositioning
- Skin tightening
2. Patients seeking subtle or “trial” enhancement
- Unsure about permanent change
- Prefer reversible options
Start with fillers to simulate projection first.
3. Very thick soft tissue envelope
- Can blunt implant definition
- May require larger implant ? risk of overcorrection
 Can blunt implant definition
Can blunt implant definitionPoor Candidates (Who should NOT get them)
1. Normal or already prominent midface
- Adequate or strong projection already
- Risk: unnatural “overfilled” or “protrusive” look
2. Wide bizygomatic face with lateral cheek prominence
- Common in some Asian facial types
- Adding volume laterally worsens facial width
 Common in some Asian facial types
Common in some Asian facial typesThese patients often need:
- Reduction (zygoma reduction), not augmentation
3. Unrealistic aesthetic expectations
- Want dramatic transformation beyond anatomical limits
- Desire “Westernization” without regard for facial harmony
 Desire “Westernization” without regard for facial harmony
Desire “Westernization” without regard for facial harmony4. Poor understanding of permanence
- Especially important with:
- Porous implants (Medpor)
- PEEK implants
5. Active infection or poor oral hygiene
- Intraoral approach increases infection risk
 Intraoral approach increases infection risk
Intraoral approach increases infection risk6. Medical contraindications
- Poor healing capacity
- Immunocompromised states
- Smoking (relative risk factor)
Key Clinical Decision Framework
 Comprehensive preoperative evaluation includes:
Comprehensive preoperative evaluation includes:
1. Profile analysis (most important)
- Is the midface retrusive relative to:
- Forehead
- Lower face?
2. Infraorbital–cheek junction
- Smooth vs hollow vs step-off
3. Paranasal support
- Nasolabial angle
- Base of nose projection
4. Facial width vs projection balance
- Especially critical in Asian patients:
- Avoid increasing width
- Focus on forward projection
Simple Rule of Thumb
- Flat + hollow + forward deficiency ? GOOD candidate
- Full + wide + only wants contour ? BAD candidate
- Aging-only problem ? WRONG procedure
Dr. Barry Eppley
Plastic Surgeon