


Frontal hairline advancement (also called forehead reduction surgery) is a procedure that physically moves the hairline forward to reduce the height of the forehead.
How it works
- A surgeon makes an incision along the natural hairline
- The forehead skin is advanced downward
- The hair-bearing scalp is brought forward and sutured in place
- Excess forehead skin is removed
This results in an immediate lowering of the hairline (unlike hair transplants, which take months to grow in).
Typical results
- Hairline lowered by about 1–3 cm in one procedure
- Immediate visible change
- Scar is usually placed at the hairline and can be well concealed over time
Who is a good candidate
- High forehead or naturally high hairline
- Good scalp laxity (loose scalp that can move forward)
- Stable hair loss pattern (important—ongoing recession can affect results)
How it compares to a hair transplant
Hairline advancement:
- Immediate result
- Moves entire hairline forward
- Better for large forehead reduction
Hair transplant:
- Gradual (6–12 months)
- Adds density and refines shape
- Better for thinning or mild recession
Often, people combine both:
- Advancement for position
- Transplant later for refinement
Risks and considerations
- Visible scar (usually fine but important to consider)
- Temporary numbness of the scalp
- Hair shock loss near incision (often temporary)
- Not ideal if you have progressive male pattern baldness without stabilization
Key limitation
This surgery does not stop future hair loss. If your hairline continues to recede, the result can look unnatural over time unless managed (e.g., with medication or transplant).
Case Study

 This female had a very high hairline at 9.5cms at the central glabellar area and 8.5cms at mid-eyebrow. She also had a midline bony metopic ridge she wanted reduced. She had darkly pigmented skin and her scalp had limited mobility of 1cm.
This female had a very high hairline at 9.5cms at the central glabellar area and 8.5cms at mid-eyebrow. She also had a midline bony metopic ridge she wanted reduced. She had darkly pigmented skin and her scalp had limited mobility of 1cm.
 Under general anesthesia a frontal hairline incisions was made from one mid-temporal hairline to the other. The frontal scalp edge on the bone was marked for reference. The forehead flap was elevated in the midline to the metopic ridge reduction.
Under general anesthesia a frontal hairline incisions was made from one mid-temporal hairline to the other. The frontal scalp edge on the bone was marked for reference. The forehead flap was elevated in the midline to the metopic ridge reduction.
 The entire scalp was elevated at the subgaleal level over the bone centrally and on top of the deep temporal fascia on the sides. Three levels of galeal releases were done from side to side The scalp was advanced over the forehead skin and the skin was marked as to how far forward it could move. This marked the amount of forehead skin reduction that could be achieved.
The entire scalp was elevated at the subgaleal level over the bone centrally and on top of the deep temporal fascia on the sides. Three levels of galeal releases were done from side to side The scalp was advanced over the forehead skin and the skin was marked as to how far forward it could move. This marked the amount of forehead skin reduction that could be achieved.

 The forehead skin was excised and the advanced scalp secured centrally to its upper edge with suture fixation of the galea to micro screws into the bone. With secure galeal fixation of the advanced scalp flap a two layer resorbabe suture closure was done. This reduced the forehead length central to 7cms for a 2.5cm advancement.
The forehead skin was excised and the advanced scalp secured centrally to its upper edge with suture fixation of the galea to micro screws into the bone. With secure galeal fixation of the advanced scalp flap a two layer resorbabe suture closure was done. This reduced the forehead length central to 7cms for a 2.5cm advancement.
Discussion
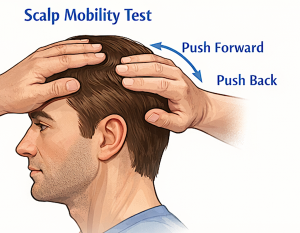
Scalp laxity is one of the most important factors in determining how much a hairline can be advanced. Surgeons assess it both manually and, less commonly, with measuring devices.
1. Manual (most common method)
This is what almost every surgeon does in clinic.
Forward–backward mobility test
- The surgeon places fingers on your scalp (usually top or sides of the head)
- They push the scalp forward toward the forehead and then backward
 They assess:
They assess:
- How far it moves
- How easily it moves (tight vs loose)
 They assess:
They assess:
? This gives a quick sense of whether you have:
- Good laxity = more advancement possible
- Tight scalp = limited advancement
“Pinch test”
- The surgeon pinches the scalp between fingers
- Measures how much tissue can be lifted away from the skull
More “pinchable” tissue = more flexibility to advance
2. Measurement in centimeters (practical estimation)
Some surgeons will actually quantify it:
- They push the hairline forward as far as it comfortably goes
- Then measure the distance from the original hairline to the pushed position
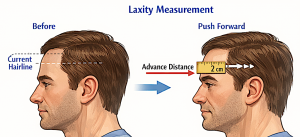 Then measure the distance from the original hairline to the pushed position
Then measure the distance from the original hairline to the pushed positionExample:
- If your hairline can be pushed forward 1.5–2 cm, that’s roughly your maximum safe advancement
3. Elasticity vs laxity (subtle but important)
Surgeons are also judging:
- Elasticity = how well the scalp stretches
- Laxity = how much it can move overall
You can have:
- Good stretch but limited movement (less ideal)
- Or good mobility (ideal for surgery)
4. Advanced tools (less common)
Some clinics use devices like a laxometer, which:
- Applies controlled tension
- Measures displacement in millimeters
These are more common in research or hair transplant planning, but not necessary for most cases.
5. Why this matters surgically
Scalp laxity determines:
- How many centimeters the hairline can be lowered
- Whether you need:
- Single-stage advancement (good laxity)
- OR tissue expansion first (tight scalp)
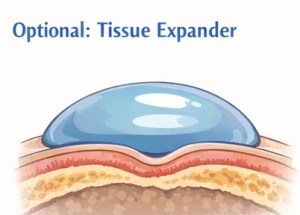
6. Tissue expansion (if laxity is low)
If your scalp is tight:
- A balloon-like expander is placed under the scalp
- Gradually inflated over weeks
- Creates extra skin so more advancement is possible later
 A balloon-like expander is placed under the scalp
A balloon-like expander is placed under the scalpSimple rule of thumb
- Loose scalp ? bigger, safer advancement
- Tight scalp ? limited movement or staged approach
Dr. Barry Eppley
Plastic Surgeon