

 A negative orbital vector (NOV) describes the relationship between the globe (eyeball) and the infraorbital rim (the cheekbone beneath the eye). In NOV, the eye projects further forward than the supporting bone.
A negative orbital vector (NOV) describes the relationship between the globe (eyeball) and the infraorbital rim (the cheekbone beneath the eye). In NOV, the eye projects further forward than the supporting bone.
This can result in:
- Tear trough hollowing
- Lower eyelid retraction or increased scleral show
- Higher risk of lower eyelid malposition after blepharoplasty
- A fatigued or skeletonized facial appearance
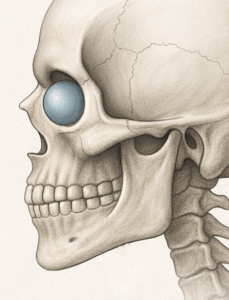
3D CT Findings in NOV

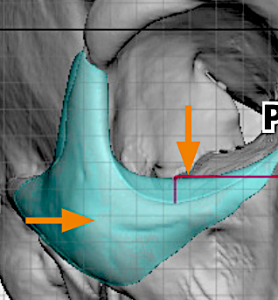
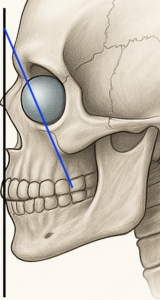 While NOV is most commonly described by the external relationship between the eyeball and the sot tissue fullness over the infraorbital rim and cheek tissues the bone shape changes ion a 3D CT scan are also evident. The classic profile finding is the significant retrusion of the infraorbital rim/zygomatico-maxillary (ZMC) complex. This retrusion is usually almost 45 degrees or greater from the vertical facial axis.
While NOV is most commonly described by the external relationship between the eyeball and the sot tissue fullness over the infraorbital rim and cheek tissues the bone shape changes ion a 3D CT scan are also evident. The classic profile finding is the significant retrusion of the infraorbital rim/zygomatico-maxillary (ZMC) complex. This retrusion is usually almost 45 degrees or greater from the vertical facial axis.

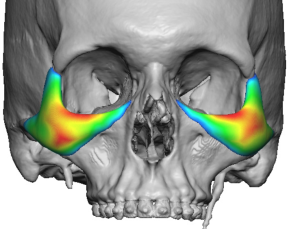
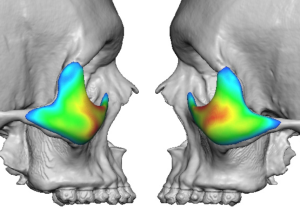
 But there are also skeletal indicators in the front view as well. The vertical length between the supraorbital and infraorbital rims is elongated and the lateral infraorbital rim swoops downward. In the submental view the retrusion of the ZMC complex is evident with an inward displacement.
But there are also skeletal indicators in the front view as well. The vertical length between the supraorbital and infraorbital rims is elongated and the lateral infraorbital rim swoops downward. In the submental view the retrusion of the ZMC complex is evident with an inward displacement.
Limitations of Common Treatments
The most frequently used treatments for NOV are injectable fillers and fat grafting. However, these approaches have significant limitations:
- Results are temporary
- Outcomes are often inconsistent
- They do not correct the underlying skeletal deficiency
NOV is fundamentally not a soft tissue problem—the soft tissue changes are secondary to inadequate bony support.
Role of Implants
Implants play a central role in correcting skeletal deficiencies. They are particularly useful when:
- Osteotomies are not appropriate
- Onlay bone grafting is insufficient or impractical
Goals of Implant Treatment
- Augment the infralateral orbital rim
- Improve the globe-to-rim relationship
- Provide structural support to the lower eyelid
- Reduce scleral show and tear trough depth
Standard Implant Option
Tear Trough Implants
Originally designed for age-related grooves along the medial infraorbital rim, these implants:
- Provide horizontal projection along the infraorbital rim
- Do not increase vertical rim height
- Offer limited lateral orbital rim coverage
- Are commonly placed via a transconjunctival approach
While widely used, they are often insufficient for NOV correction due to the three-dimensional nature of the deformity with a limited 2D implant. Only in cvery mild cases are theyt usually effectice.
Advantages of Custom Implants
Standard implants frequently fall short because NOV is a complex, three-dimensional, patient-specific problem.
Custom (patient-specific) implants:
- Are designed from CT scan data
- Precisely match orbital rim curvature and asymmetry
- Can extend into multiple regions, including:
- Infraorbital rim
- Pyriform aperture
- Maxilla
- Allow controlled forward projection where needed
Key Concept
NOV is fundamentally a skeletal support deficiency. Custom implants provide one of the most definitive solutions by restoring orbital support in a unified, three-dimensional manner.
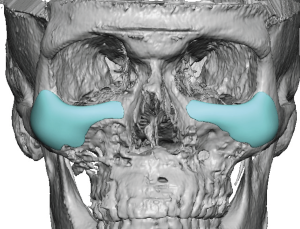
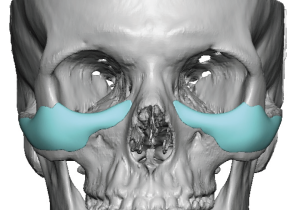
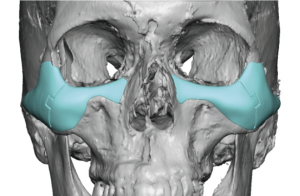
Eppley-Style Custom Implants for NOV
The core principle is not simply augmenting the infraorbital rim, but reconstructing the entire midface support platform in a continuous, anatomically blended way.
Core Design Philosophy
- Treat NOV as a global skeletal deficiency rather than a localized defect
- Create a smooth, continuous augmentation from:
- Medial infraorbital rim ? central rim ? lateral rim
- Extend inferiorly and laterally onto the cheek
- Avoid step-offs or isolated projection that appears unnatural
Implant Design Components (Single Integrated Piece)
1. Infraorbital Rim Augmentation
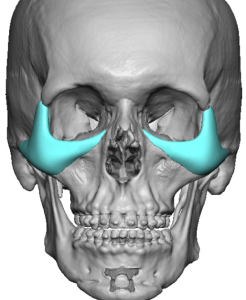
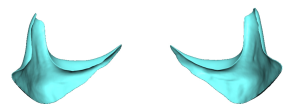
- Saddles the infraorbital rim
- Adds both vertical height and horizontal projection
- Produces a superoanterior (3D) expansion of the rim
- Enhances lower eyelid support
- May be combined with soft tissue procedures (e.g., spacer grafts)
2. Medial Extension (Nasal Region)
- Extends toward the nasal bones
- Improves correction of medial tear trough deformity
- Prevents a segmented or disconnected appearance
3. Inferior Extension
- Extends below the infraorbital rim while avoiding the infraorbital nerve
- Positioned more laterally relative to the nerve
- Provides vertical support at the lid–cheek junction
- Softens the transition from a negative to a more neutral vector
4. Lateral Extension (Zygomatic Transition)
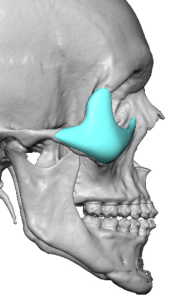
- Blends into the malar eminence
- Prevents a central over-projection or “bulge”
- Ensures a smooth transition into the lateral orbit
- May extend onto the zygomatic arch when needed for continuity
Shape and Surface Characteristics
Contouring
- Fully customized based on CT anatomy
- Accounts for asymmetry, rim depth, and globe position
Feathered Edges
- Minimize palpability and visibility
- Especially important along inferior and lateral borders
Thickness Gradient
- Maximum thickness at the infraorbital–cheek junction
- Gradual tapering medially, laterally, and inferiorly
Vector Correction Strategy
Rather than simply adding volume, the implant is designed to reposition skeletal support:
- Converts a negative vector to neutral or slightly positive
- Advances the infraorbital support structure to match or exceed globe projection
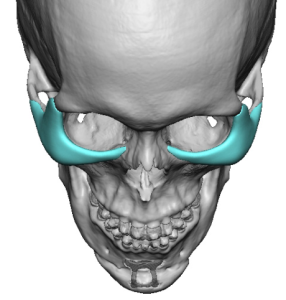
Fixation and Stability

- Screw fixation at the infraorbital rim and upper cheek
- Custom fit enhances positioning accuracy
- Orbital rim “saddling” improves stability and reproducibility
Surgical Access

- Typically placed through a subciliary (lower eyelid) incision, critical for an implant that saddles the rim
- Intraoral access used when significant maxillary extension is required
- Implant design considers insertion pathway
- May be fabricated as a multi-piece design for safe placement
Design Variations by Severity
Mild NOV
- Rim-focused implant
- Minimal cheek extension
Moderate NOV
- Rim plus cheek extension
- Moderate inferior/maxillary extension
Severe NOV
- Full upper midface wraparound design
- Strong cheek augmentation
- Lateral arch extension
- Greater inferior maxillary expansion
Distinguishing Features of Eppley-Style Implants
- Broader anatomical footprint beyond the orbital rim
- Emphasis on rim “saddling” for structural integration
- Designed for aesthetic blending, not just augmentation
Common Pitfalls Avoided
- Isolated rim augmentation that creates an unnatural shelf
- Failure to address the cheek, leading to incomplete correction
- Sharp or poorly blended edges that are visible or palpable
Final Takeaway
Eppley-style custom implants for NOV function as comprehensive midface augmentation system, not isolated orbital implants.
They:
- Rebuild the skeletal platform beneath the eye
- Restore proper support and contour
- Improve lid–cheek harmony
They are frequently combined with adjunctive lower eyelid procedures (e.g., canthopexy, canthoplasty, spacer grafts) to optimize both structural support and soft tissue position.
Dr. Barry Eppley
Plastic Surgeon