


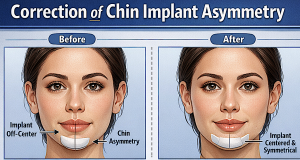
Chin implant asymmetry is a well known aesthetic complication and can arise from implant malposition, soft tissue differences, bony asymmetry, lack of secure fixation or other healing-related factors. Surgical correction depends on identifying the exact cause.
Common Causes
- Implant malposition (most common): shifted, rotated, or not centered
- Incorrect implant size/shape
- Underlying bony asymmetry
- Soft tissue imbalance or mentalis muscle issues
- Capsular contracture (scar tissue tightening around implant)
Surgical Correction Options
1. Implant Repositioning
- Most straightforward fix if implant has shifted
- Pocket is reopened, implant centered, and secured
- The use of screw fixation is mandatory to prevent recurrence
2. Implant Exchange
- Replace with a better-fitting implant (different size, shape, or style)
- Extended anatomical implants are the most common cause of asymmetry die to their long wings
3. Pocket Modification
- Adjusting the implant pocket:
- Release the constricted side
- Critical for preventing repeat displacement
4. Capsulectomy/Capsulotomy
- Removal of scar capsule if it’s causing distortion
- Often combined with repositioning or replacement
5. Addressing Bony Asymmetry
- If underlying chin bone is asymmetric:
- Implant alone may not work well
- Bony overgrowths and irregularities are common around chin implants and must be removed in chin implant revisions/replacements
6. Soft Tissue Balancing
- Mentalis muscle resuspension
- Fat grafting for contour refinement if mild asymmetry remains
Implant Revision vs. Sliding Genioplasty
- Implant revision: simpler, less invasive, good for positional issues
- Sliding genioplasty: conversion considered if patient so desires or after multiple ‘failed’ chin implant surgeries
?? Key Surgical Principles
- Precise midline identification is critical
- Avoid over-dissecting the pocket (prevents drifting)
- Screw fixation techniques is essential in revision cases
- Symmetry should be judged in 3D, not just frontal view
Practical Insight
In revision cases, the biggest mistake is just “re-centering” the implant without correcting the underlying cause (e.g., asymmetrical pocket or bone). That’s why recurrence happens.
Case Example

 This female had a history of two chin implant surgeries with an extended anatomic silicone chin implant. The first was through a submental incision with resultant asymmetry. A second surgery for revision was done intraorally with ‘bone removal’ on the left side. Persistent implant asymmetry remained with the left wing of the implant lower than the inferior border and the right wing higher with a visible external tilt to the implant. In addition she never liked the chin implant because it made her lower face to wide.
This female had a history of two chin implant surgeries with an extended anatomic silicone chin implant. The first was through a submental incision with resultant asymmetry. A second surgery for revision was done intraorally with ‘bone removal’ on the left side. Persistent implant asymmetry remained with the left wing of the implant lower than the inferior border and the right wing higher with a visible external tilt to the implant. In addition she never liked the chin implant because it made her lower face to wide.
 As a third chin implant surgery through her existing submental scar her extended chin implant was removed, the capsules were elevated off of the bone and any bony overgrowths were removed with an osteotome. The removed chin implant could be seen being an extended style with 7 mm of horizontal projection and the ends of the wings bluntly cut off. Then a standard silicone chin implant was modified by removing its wings as well as tapering it to give it a less round shape.
As a third chin implant surgery through her existing submental scar her extended chin implant was removed, the capsules were elevated off of the bone and any bony overgrowths were removed with an osteotome. The removed chin implant could be seen being an extended style with 7 mm of horizontal projection and the ends of the wings bluntly cut off. Then a standard silicone chin implant was modified by removing its wings as well as tapering it to give it a less round shape.
 It was then inserted in position in the midline and secured with two micro screws on each side.
It was then inserted in position in the midline and secured with two micro screws on each side.
 The immediate effects showed symmetric chin implant placement with a much less wide chin shape.
The immediate effects showed symmetric chin implant placement with a much less wide chin shape.
Discussion
Revision chin implant surgery is where small technical errors create repeat problems. Here are the most common pitfalls—these are the ones that lead to persistent asymmetry or recurrence: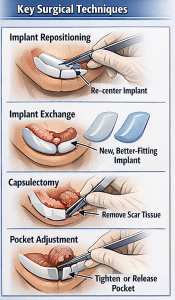
?? 1. Treating the Symptom, Not the Cause
- Simply re-centering the implant without diagnosing why it was off
- Missed issues:
- Asymmetric pocket
- Bony asymmetry
- Muscle pull (mentalis)
- Fix: Always identify the primary driver before revising.
?? 2. Inadequate Pocket Control
- Over-dissected pocket ? implant drifts again
- Failure to tighten the “loose side”
- Not releasing the “tight side”
- Fix: Create a precisely balanced pocket, often asymmetric by design
?? 3. Ignoring Capsular Contracture
- Leaving scar capsule intact when it is deforming implant position
- Leads to persistent deviation or relapse
- Fix: Perform partial or complete capsulectomy when indicated
?? 4. Wrong Implant Selection (Again)
- Replacing with the same style/size implant
- Not accounting for asymmetry (using symmetric implant in asymmetric anatomy)
- Fix:
- Consider custom implant design or modifying a standard chin implant for better fit
?? 5. Failure to Address Bony Asymmetry
- Trying to “camouflage” skeletal asymmetry with an implant
- Leads to persistent off-center appearance even if implant is centered
- Fix: Get 3D CT scan to fully see the underlying bone shape and design an implant that fits better
?? 6. Poor Midline Assessment
- Using soft tissue landmarks (which may be asymmetric)
- Not referencing true skeletal midline
- Fix:
- Use dental midline + skeletal landmarks
- Evaluate in frontal and basal views
?? 7. No Implant Fixation in Revision Cases
- Implant allowed to float in a previously unstable pocket
- Higher risk of repeat shifting
- Fix:
- Use screw fixation in revisions
?? 8. Mentalis Muscle Mismanagement
- Failure to properly resuspend/tighten mentalis
- Leads to:
- Chin ptosis
- Asymmetric animation
- Fix: Careful layered closure and muscle reattachment
?? 9. Underestimating Soft Tissue Asymmetry
- Even with perfect implant position, soft tissue can create asymmetry
- Fix:
- Fat grafting
- Limited contour adjustments
?? 10. Inadequate Preoperative Analysis
- No visualization of implant with 3D CT scan
- No photographic evaluation in complex cases
- Fix:
- Analyze in 3D
- Use imaging in every revision case
? High-Yield Takeaway
Most failed revisions happen because the surgeon repeats the same operation without fully understanding the problem. The solution may not be as simple as simply ‘re-centering’ the implant.
Dr. Barry Eppley
Plastic Surgeon