


Forehead osteomas are benign (non-cancerous) bone tumors that commonly appear on the frontal bone of the skull—basically the forehead area.
What they are
- Made of dense, mature bone
- Typically slow-growing
- Feel like a hard, immovable lump under the skin
- Usually painless
Why they occur
The exact cause isn’t always clear, but possible factors include:
- Genetics (sometimes seen in conditions like Gardner’s syndrome, though most cases are isolated)
- Prior trauma (occasionally)
- Developmental bone growth abnormalities
Symptoms
Most people notice:
- A visible bump on the forehead
- Firm, smooth, round or oval shape
- No redness or tenderness
They’re usually cosmetic concerns, not medical problems.
Diagnosis
- Often diagnosed by physical exam
- CT scan is the gold standard if confirmation is needed (shows dense bone growth)
Treatment
Not required unless bothersome. Options include:
1. Observation
- If small and not noticeable
2. Surgical removal (most common)
- Done for cosmetic reasons
- Typically outpatient
- Can be performed via:
- Direct excision (small incision over lesion)
- Endoscopic approach (hidden incisions behind hairline)
Risks of removal
- Scar (usually minimal)
- Temporary swelling/bruising
- Rare: contour irregularities
When to get evaluated
- Rapid growth (unusual)
- Pain or tenderness
- Multiple lesions (may warrant further workup)
Case Example
 This middle aged female developed a slow growing hard bump in her left upper forehead. It was very firm and immobile. No x-rays were obtained as it apepare t0 be a classic osteoma.
This middle aged female developed a slow growing hard bump in her left upper forehead. It was very firm and immobile. No x-rays were obtained as it apepare t0 be a classic osteoma.

 Under anesthesia a frontal hairline incision was narked above it (red marled the osteoma). Through the fromtal hairline incision the osteoma was exposed.
Under anesthesia a frontal hairline incision was narked above it (red marled the osteoma). Through the fromtal hairline incision the osteoma was exposed.

 Using a sharp chisel the osteoma was separated from the underlying forehead bone and removed.
Using a sharp chisel the osteoma was separated from the underlying forehead bone and removed.
 The frontal hairline inision was closed with small resorbable sutures and a smooth forehead was restored.
The frontal hairline inision was closed with small resorbable sutures and a smooth forehead was restored.
Discussion
Here’s a practical, surgical comparison of open vs. endoscopic forehead osteoma removal:
Open (Direct) Excision
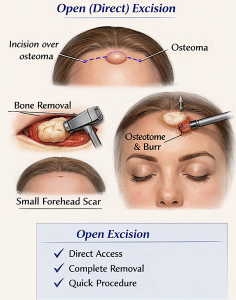
Technique
- Small incision directly over the osteoma
- Skin and soft tissue elevated
- Osteoma removed using:
- Osteotome (chisel)
- Burr (to smooth contour)
- Closure in layers
Best for
- Large osteomas
- Very hard/dense lesions
- Lesions needing precise contouring
- Patients with forehead wrinkles (scar can be hidden)
Advantages
- Direct visualization ? maximum control
- More complete removal (especially deep lesions)
- Easier to feather edges for smooth contour
- Shorter operative time
Disadvantages
- Visible scar (though often minimal)
- Slightly more soft tissue disruption
Endoscopic Removal
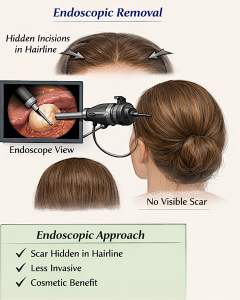
Technique
- 1–3 small incisions behind the hairline
- Endoscope inserted under the forehead soft tissue
- Subperiosteal dissection to reach osteoma
- Osteoma removed with burr or osteotome under camera visualization
Best for
- Small to medium osteomas
- Patients wanting no visible forehead scar
- Lesions located higher on the forehead
Advantages
- Scar hidden in hairline
- Less visible evidence of surgery
- Good for cosmetic-focused patients
Disadvantages
- Limited exposure
- Technically more demanding
- May be harder to fully contour large lesions
- Slightly longer operative time
- Risk of incomplete smoothing if not ideal access
Key Technical Considerations
Plane of dissection
- Typically subperiosteal for both approaches
- Protects supraorbital and supratrochlear nerves
Contouring
- Critical step: burring the base after removal
- Prevents visible step-offs or recurrence-like appearance
Nerve preservation
- Supraorbital nerve exits:
- Notch or foramen (~2.5 cm from midline)
- Must be identified/protected, especially endoscopically
? Decision Algorithm (Simplified)
- Small + patient wants no scar ? Endoscopic
- Large / very prominent ? Open
- Low forehead (near brow) ? Usually open
- High forehead (behind hairline access possible) ? Endoscopic
? Recovery Differences
|
Factor |
Open |
Endoscopic |
|
Swelling |
Mild–moderate |
Moderate (forehead elevation) |
|
Bruising |
Minimal |
Can track to eyelids |
|
Scar |
Visible but small |
Hidden |
|
Downtime |
~5–7 days |
~7–10 days |
Pearl (from a surgical standpoint)
The biggest mistake is under-contouring—leaving a subtle bump.
A slightly more aggressive burring and feathering almost always gives the best aesthetic result, regardless of approach.
Dr. Barry Eppley
Plastic Surgeon