

 Medpor jaw angle implant removal is one of the more technically demanding explant procedures because of thick soft tissue coverage, strong tissue ingrowth, and proximity to the masseter muscle and the facial artery.. It’s very different from silicone angle implant removal and often behaves like a deep subperiosteal dissection with partial reconstruction.
Medpor jaw angle implant removal is one of the more technically demanding explant procedures because of thick soft tissue coverage, strong tissue ingrowth, and proximity to the masseter muscle and the facial artery.. It’s very different from silicone angle implant removal and often behaves like a deep subperiosteal dissection with partial reconstruction.
Here’s how it’s typically approached and what makes it unique:
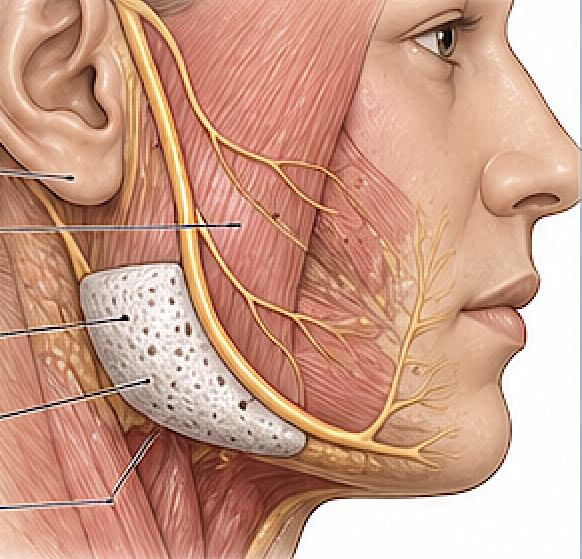
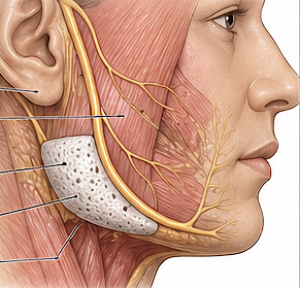
? Key Anatomical Challenges (Jaw Angle)
- Facial artery (most critical risk)
- Masseter muscle (implant often partially embedded)
- Pterygomasseteric sling
- Thick periosteum and dense soft tissue
- Limited exposure compared to chin/cheek
? Surgical Approach
1. Incision Choice
Most commonly:
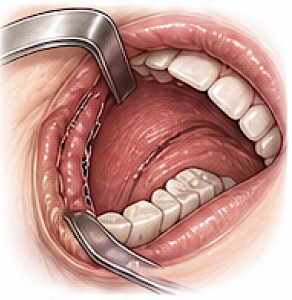
- Intraoral (posterior vestibular incision)
- Avoids external scar
- More difficult exposure
- Can not see the bottom of the implant…where all the risk issues reside
Less commonly:
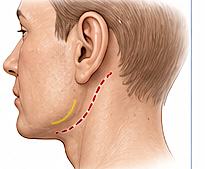
- External (submandibular/retroauricular)
- Used in:
- When such an existing incisions exists as out was initially placed that was
- Better preservation of masseter muscle/ptergo-masseteric sling
- Need for wide exposure along the bottom of the implant
- Used in:
2. Subperiosteal Elevation
- Elevation along:
- Mandibular ramus ? angle ? posterior body
- Key principle:
- Stay on bone initially to avoid muscle disruption/ injury
- Easiest tissue plane to elevate since no bone ingrowth occurs
3. Identification & Protection of Masseter Muscle
Techniques:
- Sharp dissection on external and bottom surface of implant
- Avoid:
- Aggressive inferior blind dissection on bottom of implant as the facial artery crosses the inferior border of the mandible at the angle-body junction
- If external approach:
- Better visualization of the underside of the implant and ligation of the facial artery should njury to it occur
Risk:
- Temporary severe bleeding, controlled by ligation
- Masseteric muscle dehiscence if it did not exist before
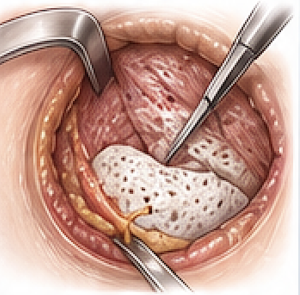
4. Piecemeal Implant Removal (Almost Always)
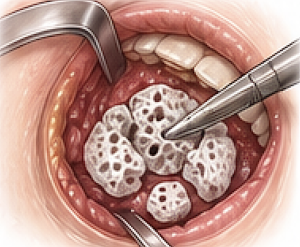
- Medpor Jaw angle has thick and highly integrated tissue ingrowth
- Technique:
- Dissect free in segments and sequentially remove.
- Only remove what you know is adequately dissected free and can be visualized
- Each implant segment removed allows more oif the implant to be seen and safely removed.
- Tools:
- Sharp elevators
- Needle point electrocautery
- Osteotomes
5. Screw Removal
- Almost all Medpor jaw angle implants will have multiple screws for fixation
- If done intraorally remove implant around the screws to expose their long threaded shaft and then turn them out by a needle holder
- If done externally use a screwdriver and remove in conventional manner
6. Hemostasis in a Vascular Field
- Masseter + ingrowth = significant bleeding
- Use:
- Electrocautery
- Maintain:
- Clear visualization at all times
7. Bone and Contour Management
After removal:
- Common findings:
- Irregular angle contour
- Mild resorption
- Management:
- Large bony overgrowths can be removed
- Imprint of the bone is not necessary to treat
6. Soft Tissue Considerations
- After implant removal:
- Loss of projection at angle
- Possible soft tissue sagging
Management options:
- Await secondary assessment after full healing at which time options include::
- Fat grafting
- New implant
- Jowl-neck tuck
0. Drain Placement (Often Recommended)
- Due to:
- Dead space
- Muscle dissection
- Helps prevent:
- Hematoma
- Seroma
? Unique Risks in Jaw Angle Medpor Removal
1. Masseter Muscle Dehiscence
- Jaw angle soft tissue contour deformity, may take months to fully see
- May be worse after implant removal if it existed before
- Can be prevented or treated with an external approach only
2. Residual Implant Fragments (rare)
- May be intentionally left if adherent to artery
- Most commonly small retained implant pieces occur because they could not be seen or found
3. Prolonged Swelling
- Jaw angle region swells more and persists longer than the chin and cheek areas
? Practical Surgical Philosophy
- Try and remove every implant fragment
- Be prepared to fragment for removal, don’t avulse
- Preserve masseter muscle as much as possible
- Be aware of the facial artery location and dissect accordingly
? Compared to Other Medpor Locations
Jaw angle removal is:
- Much harder than chin or cheek
- More challenging than initial implant placement
Dr Barry Eppley
Plastic Surgeon