

Head shape is an aesthetic feature that is often overlooked or disregarded…unless one has a head shape that they do not like. While the shape of the head does usually play second fiddle to the shape of one’s face, they are inter related and the appearance of one can affect the other. Many assume that the shape of the face is the same as that of the head, and in many people this is true, but it is not always so.
One aesthetic head feature is that of width. The width of the head is largely perceived as the bitemporal width. At its widest this is an area just about the ear from each side of the head. This is composed largely of the temporal bone and a portion of the anterior parietal bone and the posterior portion of temporalis muscle. This occupies the space from the base of the ear vertically upward to the anterior temporal line where the muscle transitions into more horizontally oriented skull bone.
While craniometry has numerous numbers for normal head width, this is as much a personal aesthetic judgment as any measurement. Heads that are seen as too wide all have a convexity to their shape that usually impinges on a vertical line that extends upward from the top of the ear. Many assume that this is due to the shape and thickness of the underlying temporal bone. But the reality is that the thickness of the muscle usually plays a more major role in the shape and thickness of the side of the head that does the bone. The location and thickness of the temporal muscle in its more posterior origin above and behind the ear is frequently underappreciated.
Aesthetic reduction of excessive temporal width, or a wide head, is often most effectively done by a temporal muscle reduction technique. Removing the posterior portion of the temporalis muscle can change the shape of the side head quite dramatically.The addition of bone reduction underneath it can be done at the same time but it has a more minimal reduction effect than that of the muscle
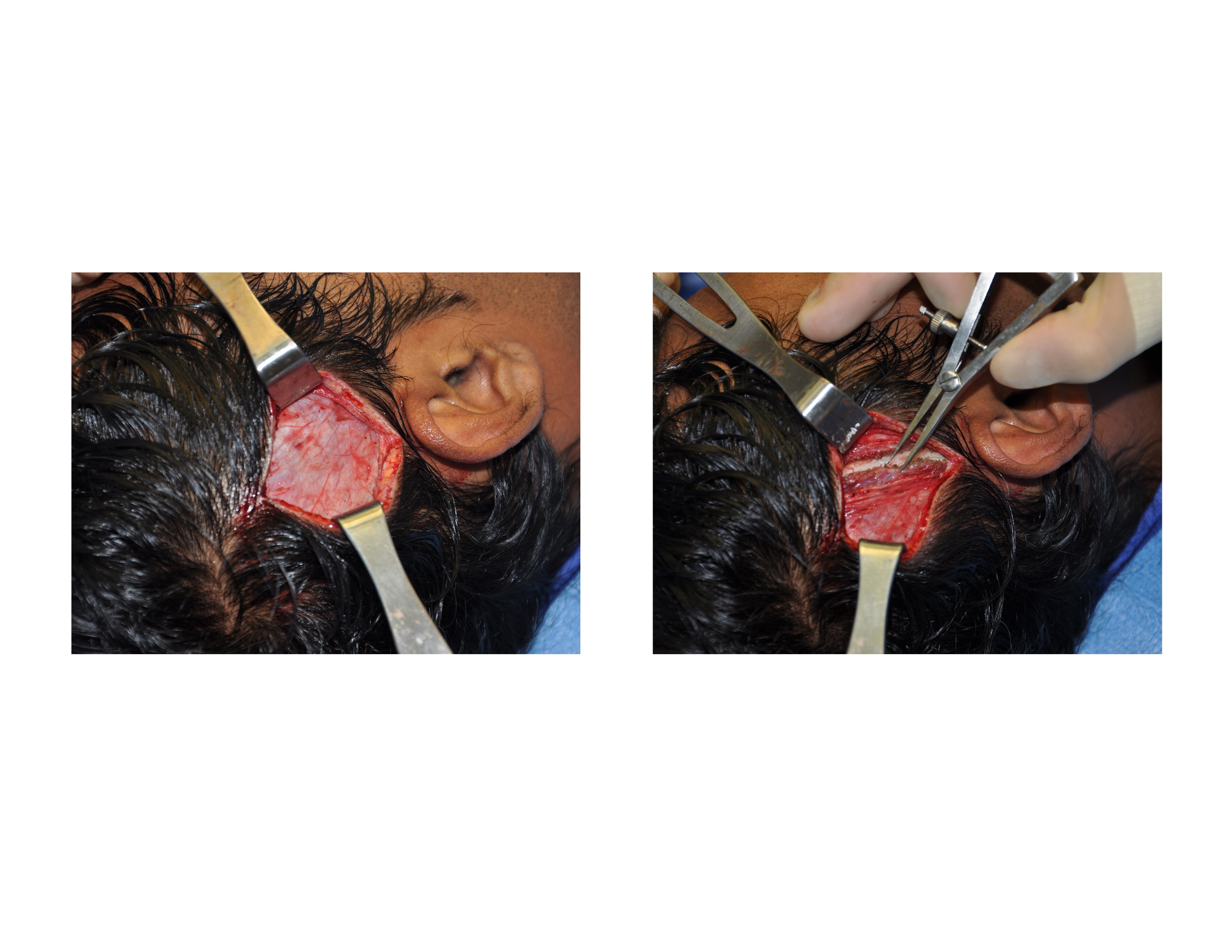 The surgical technique for aesthetic temporal reduction is done through a vertical scalp incision above the ear that has a length of no more than 7 cms. Hair is not shaven to make the incision, it is just parted by making it wet. The incision parallels the hair follicles and goes down to the galea. The galea is incised with electrocautery and the deep temporalis fascia plane exposed.
The surgical technique for aesthetic temporal reduction is done through a vertical scalp incision above the ear that has a length of no more than 7 cms. Hair is not shaven to make the incision, it is just parted by making it wet. The incision parallels the hair follicles and goes down to the galea. The galea is incised with electrocautery and the deep temporalis fascia plane exposed.
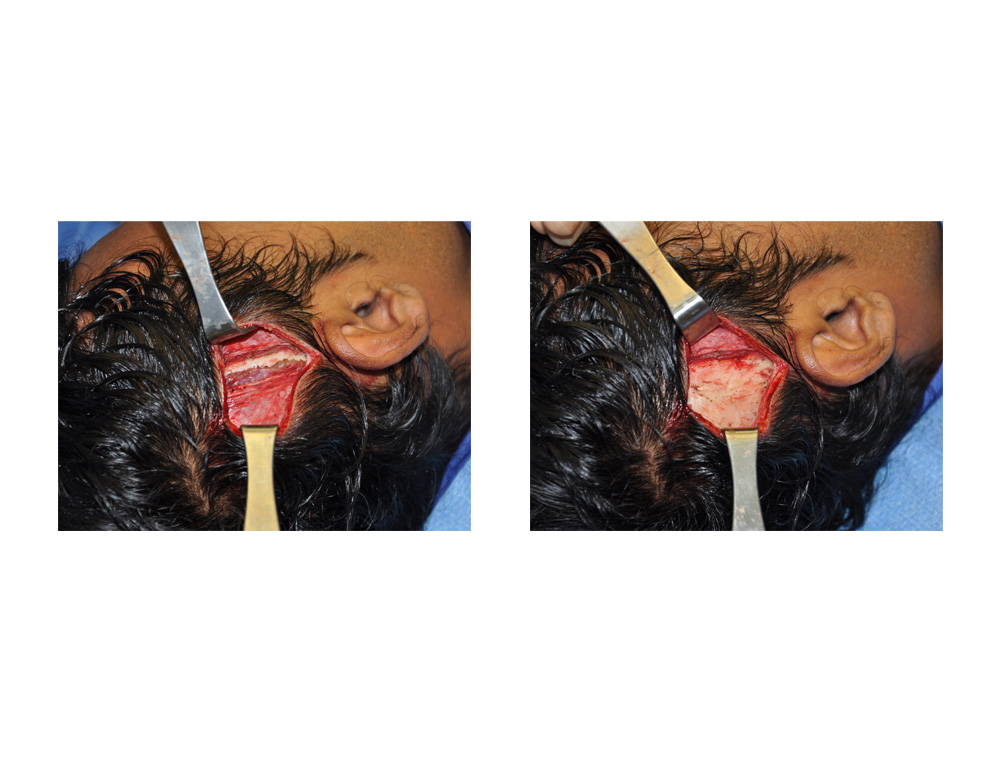 The thickness of the temporalis muscle is usually between 5 to 7mms including the fascia. But in really convex head widths, it can be even thicker. With electrocautery in an oblique orientation from the ear going upward toward the anterior temporal line, the muscle incised all he way down to the bone. From there on back the entire posterior muscle is removed. The edges of the cut muscle are cauterized so they retract back under the fascia along the open edge. When done bilaterally, the reduction in bitemporal width can be between 1 to 1.5 cms. and the side of the head shape changed from convex to a perfectly straight line.
The thickness of the temporalis muscle is usually between 5 to 7mms including the fascia. But in really convex head widths, it can be even thicker. With electrocautery in an oblique orientation from the ear going upward toward the anterior temporal line, the muscle incised all he way down to the bone. From there on back the entire posterior muscle is removed. The edges of the cut muscle are cauterized so they retract back under the fascia along the open edge. When done bilaterally, the reduction in bitemporal width can be between 1 to 1.5 cms. and the side of the head shape changed from convex to a perfectly straight line.
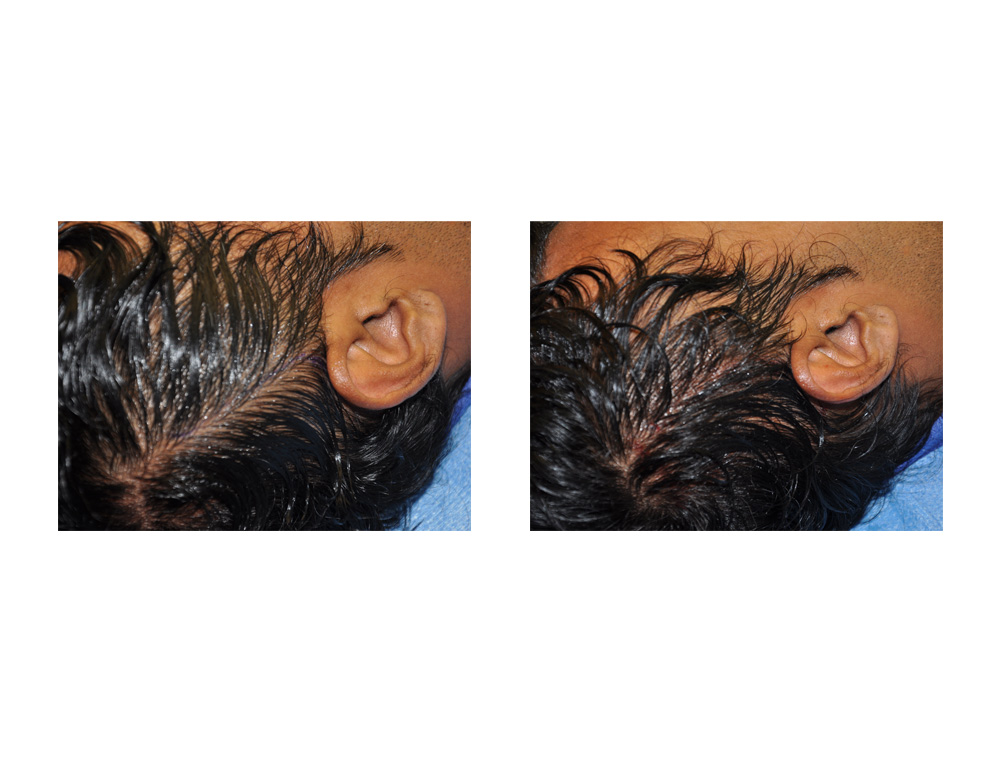 The temporal scalp skin is then closed in two layers, galea and skin. Small resorbable sutures are used and the hair combed back over the incision, making it an undetectable incision line.
The temporal scalp skin is then closed in two layers, galea and skin. Small resorbable sutures are used and the hair combed back over the incision, making it an undetectable incision line.
The logical questions about posterior temporalis muscle removal are functional in nature…if we don’t need it why is it there? As it turns out there are no functional issues caused by its excision. No patient having the procedure has had any mouth opening or closing problems. In fact not one has even had any slight pain on jaw movement. It appears that the much larger anterior portion of the temporalis muscle is the real work horse of jaw function.
Aesthetic reduction of the sides of the head can be safely and effectively done by removal of the underlying temporalis muscle. It is a very simple procedure that can be done in one hour under general anesthesia. There is minimal recovery and very little discomfort afterward.
Dr. Barry Eppley
Indianapolis, Indiana