

In rhinoplasty there are numerous features of the nose that can be reshaped. Some of these are of major size while others are comparatively small. Small size in rhinoplasty surgery, however, does not make it aesthetically insignifcant. One such small nasal feature is tknown as alar flare. This should not be confused with nasal base width which is located more inferiorly at the alar-facial groove. Reducing the amount of alar flare is a not uncommon procedure that is usually performed as the final step in rhinoplasty after the nasal incisions are closed due to the potential effects of tip manipulation on the appearance of alar flare..
Because alar flare reduction is an excision technique, it is irreversible. There are numerous technique to perform it. Choosing the correct alar excision technique and balancing that with the scar burden that results from its use is another one of the many finesse procedures in rhinoplasty.
In the November 2017 journal issue of Plastic and Reconstructive Surgery an article was published entitled ‘Managing Alar Flare in Rhinoplasty.’ In this paper the authors highlight the following important concepts of surgical alar flare reduction.
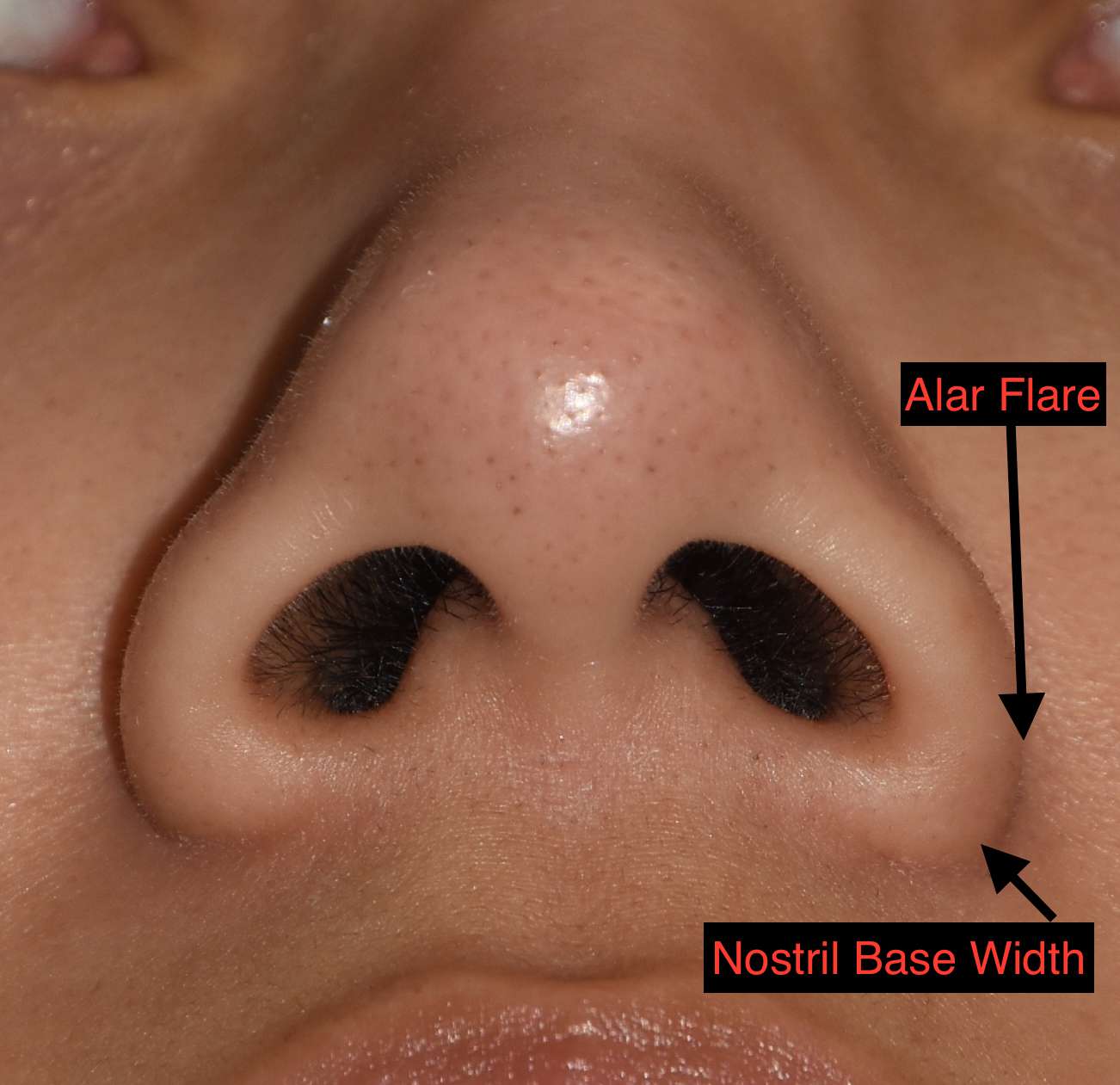 Alar flare and nasal base width should not be confused as they are not interchangeable terms. Alar flare is the most lateral projection of the alar rim. This may or may not be equal to the alar base. Limited alar flare of a few millimeters is common.
Alar flare and nasal base width should not be confused as they are not interchangeable terms. Alar flare is the most lateral projection of the alar rim. This may or may not be equal to the alar base. Limited alar flare of a few millimeters is common.
Alar flare is classified into three types based on how the lateral part of the alar rim (LAR) is vertically located relative to the nasal sill-base junction (NSBJ) in the submental view. Type 1 = LAR < NSBJ, Type 2 = LAR = NSBJ and Type 3 LAR > NSBJ.
Reduction of alar flare can be done by excision of alar lobular skin with an important goal of minimizing scar visibility and matching the excision technique to the alar flare type.
 Type 1 alar flare is managed by a limited obliquely-oriented skin excision just above the alar-facial groove.
Type 1 alar flare is managed by a limited obliquely-oriented skin excision just above the alar-facial groove.
Type 2 alar flare reduction is done with a more horizontally-oriented skin excision that is carried further up along the alar-facial groove.
Type 3 altar flare reduction uses a superiorly-oriented skin excision that extends upward to the most lateral point along the alar-facial groove.
The skin excision should be placed 1mm anterior to the alar groove.
Asymmetry is very easy to occur in alar flare reduction, like nasal width reduction, is precision of markings and detailed execution is critical to avoid it.
Some alar flare is preferable to over resection of it to avoid nostril distortion.
Very significant nose width reduction may need to combine nasal base width reduction (e.g., sill excision) with alar flare reduction.
Alar flare reduction creates a more subtle change than the more powerful techniques of nasal base width reduction.
Dr. Barry Eppley
Indianapolis, Indiana