

There are many myths and misconceptions regarding waist reduction surgery by rib removal. Most of these are based on a failure to understand the anatomy of the lower ribs and the surrounding soft tissues. Having removed hundreds of ribs for purposes of aesthetic waist reduction, I have developed insights into why rib removal has an effect on the shape of the waistline as well as how to perform it both safely and effectively.
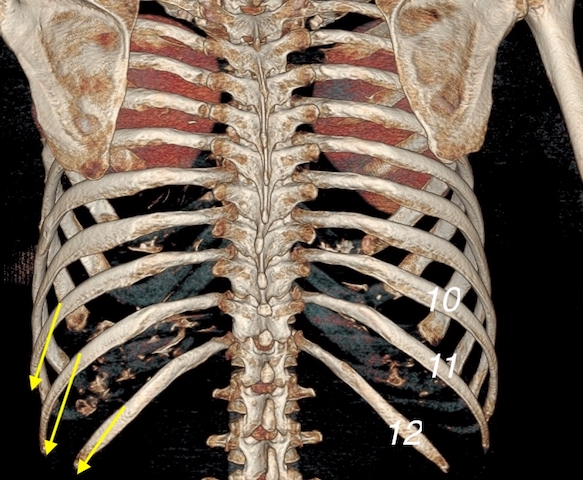
 #1 The shape of the lower ribs near the waistline is almost vertical. It is commonly perceived that the lower ribs leave the vertebrae column in a near horizontal projection and their ends stick out to the sides. But during rib removal surgery one discovers that the outer half of the ribs have a near vertical orientation. This can be appreciated in 3D CT scans of the ribcage. They start out in a somewhat horizontal orientation as they leave the spine. But out at about mid-length they turn downward to a greater than 70 degree angle. One can actually see this on the 3D CT scan as the bend starts the rib actually becomes a little thicker, undoubtably due to increased downward muscle pull.
#1 The shape of the lower ribs near the waistline is almost vertical. It is commonly perceived that the lower ribs leave the vertebrae column in a near horizontal projection and their ends stick out to the sides. But during rib removal surgery one discovers that the outer half of the ribs have a near vertical orientation. This can be appreciated in 3D CT scans of the ribcage. They start out in a somewhat horizontal orientation as they leave the spine. But out at about mid-length they turn downward to a greater than 70 degree angle. One can actually see this on the 3D CT scan as the bend starts the rib actually becomes a little thicker, undoubtably due to increased downward muscle pull.
Surgical Relevance: The lower ribs only need to be taken back at most to where the vertical bend starts. (usually the outer half) Total rib removal is unnecessary.
 #2 Rib #12 has the least influence on waist reduction. The shortest of all paired ribs is #12 at the lower end of the ribcage.This is evident on any anatomic rendering of the ribs and can be substantiated surgically. As a result, contrary to the perception of some, it is minimal influence on support of the lateral waistline. It is the most medial of the lower ribs to remove due to its shorter length. It usually can not be felt externally and what most think is rib #12 is actually rib #11 by deep palpation.
#2 Rib #12 has the least influence on waist reduction. The shortest of all paired ribs is #12 at the lower end of the ribcage.This is evident on any anatomic rendering of the ribs and can be substantiated surgically. As a result, contrary to the perception of some, it is minimal influence on support of the lateral waistline. It is the most medial of the lower ribs to remove due to its shorter length. It usually can not be felt externally and what most think is rib #12 is actually rib #11 by deep palpation.
Surgical Relevance: Only the very end of rib #12 needs to be removed, usually about 2 cms at most.
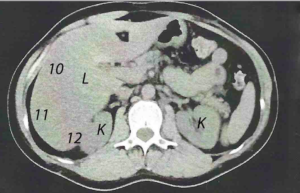 #3 The protection of the kidney by rib #12 is not affected by its shortening. The only organ close to the lower ribs is the kidney which sits behind the inner most part of rib #12. But removing just its end, which is all that is needed, does not result in loss of bony protection of the kidney. In dissecting off the attachments to the end of rib #12 some fat will occasionally be seen. This is retroabdominal fat, not perinephric fat. The fascia over the fat is closed to prevent the rare risk of a posterior abdominal wall hernia.
#3 The protection of the kidney by rib #12 is not affected by its shortening. The only organ close to the lower ribs is the kidney which sits behind the inner most part of rib #12. But removing just its end, which is all that is needed, does not result in loss of bony protection of the kidney. In dissecting off the attachments to the end of rib #12 some fat will occasionally be seen. This is retroabdominal fat, not perinephric fat. The fascia over the fat is closed to prevent the rare risk of a posterior abdominal wall hernia.
Surgical Relevance: Removal of the end of rib #12 does not result in loss of protection for the organs. (kidney)
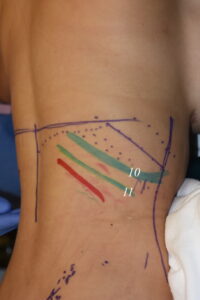 #4 Ribs #10 and 11 is what supports the lateral waistline. The longer and curved lengths of ribs #10 and #11 affects the width of the waist the most down at the level of the umbilicus. Their outer flared shape pushes out on the lateral abdominal wall. Just because rib #12 sits on the lower end of the ribcage does not mean that its reduction causes the greatest waist reduction effect.
#4 Ribs #10 and 11 is what supports the lateral waistline. The longer and curved lengths of ribs #10 and #11 affects the width of the waist the most down at the level of the umbilicus. Their outer flared shape pushes out on the lateral abdominal wall. Just because rib #12 sits on the lower end of the ribcage does not mean that its reduction causes the greatest waist reduction effect.
Surgical Relevance: Surgical efforts should be devoted to removing the maximal lengths of ribs # 10 and #11.
 #5 The cartilaginous tips of the lower ribcage provide a point of soft tissue suspension. Unlike all ribs above them, the three lower lower ribs are not attached at their ends and, as a result, have cartilaginous tips. The functional purposes of these cartilage ends is for soft tissue attachments of muscle and tendons. One of these main muscles is the internal and external oblique abdominal muscles whose insertion is on these ribs. Removing the bony end of the rib allows the cartilage tips and the muscle to collapse a bit inward.
#5 The cartilaginous tips of the lower ribcage provide a point of soft tissue suspension. Unlike all ribs above them, the three lower lower ribs are not attached at their ends and, as a result, have cartilaginous tips. The functional purposes of these cartilage ends is for soft tissue attachments of muscle and tendons. One of these main muscles is the internal and external oblique abdominal muscles whose insertion is on these ribs. Removing the bony end of the rib allows the cartilage tips and the muscle to collapse a bit inward.
Surgical Relevance: The cartilage ends of the lower ribs can be left behind and the bone disarticulated from them.
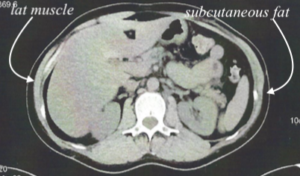 #6 The width of the waist is a combination of bony and soft tissue influences. While the support of the width of the waist certainly comes from the ribs, it is not the only contributing factor. The thickness of the subcutaneous fat layer in the adjacent flanks and the lateral projection of the thick latissimus dorsi muscle also make a contribution.
#6 The width of the waist is a combination of bony and soft tissue influences. While the support of the width of the waist certainly comes from the ribs, it is not the only contributing factor. The thickness of the subcutaneous fat layer in the adjacent flanks and the lateral projection of the thick latissimus dorsi muscle also make a contribution.
Surgical Relevance: Waist reduction surgery should incorporate soft tissue reductions with the lower rib reductions through flank liposuction and lat muscle modification at the desired maximum waist reduction area.
Dr. Barry Eppley
Indianapolis, Indiana