

The enhancement of the male chest has some obvious differences from that of the female chest. In women the goal is to make a larger mound that sits on top of the muscle. Conversely in men, the goal is to enhance the size and projection of the deeper pectoralis major muscle. As a result the resultant change in chest topography has very different desired augmentation shapes. This would indicate that not only should the size and shape of the implants needed would be different but that the created pockets would also similarly be different.
Having placed many pectoral implants and also treated numerous pectoral implant problems performed by other surgeons, there is a consistent pattern of fundamental errors in surgical technique that I have observed . They can be divided into incision placement, pocket dissection and implant shapes/dimensions.
 Like transaxillary breast augmentation in women, pectoral implants in men are placed through similar incisions. While the incision will almost always be longer than that used for breast implants, it needs to be placed high up in the axilla in a skin fold under the lateral pectoral muscle border. Some surgeons, for reasons not completely explainable, place the incision much lower along the chest wall. This makes the incision very visible and impossible to redocate. It should never be placed in this low visible location. Its only ‘advantage’ is that it makes pectoral implant revision easier particularly if pocket plication for reduction is needed.
Like transaxillary breast augmentation in women, pectoral implants in men are placed through similar incisions. While the incision will almost always be longer than that used for breast implants, it needs to be placed high up in the axilla in a skin fold under the lateral pectoral muscle border. Some surgeons, for reasons not completely explainable, place the incision much lower along the chest wall. This makes the incision very visible and impossible to redocate. It should never be placed in this low visible location. Its only ‘advantage’ is that it makes pectoral implant revision easier particularly if pocket plication for reduction is needed.
 Once of the basic differences between breast and pectoral implants is the margins of the pocket. In breast implants the effort is to make a rounder mound that needs the submuscular pocket to go behind the lateral border of the pectoral muscle to do so. (and even open up the bottom of the muscle to enable implant placement ideally centered behind the nipple) In male chest augmentation the lateral pectoral border must not be disrupted. Examination of ideal male chest shapes reinforce the precise that this is a muscle augmentation procedure and to optimally do so the implant must stay within the muscle borders. The goal is not to center the implant behind the nipple. Rather the male nipple is located at the bottom edge of the muscle/implant edge. It is not uncommon to see pectoral implants where the implant sticks out beyond the lateral muscle border, creating more of a flatter breast mound rather than a complete muscle augmentation.
Once of the basic differences between breast and pectoral implants is the margins of the pocket. In breast implants the effort is to make a rounder mound that needs the submuscular pocket to go behind the lateral border of the pectoral muscle to do so. (and even open up the bottom of the muscle to enable implant placement ideally centered behind the nipple) In male chest augmentation the lateral pectoral border must not be disrupted. Examination of ideal male chest shapes reinforce the precise that this is a muscle augmentation procedure and to optimally do so the implant must stay within the muscle borders. The goal is not to center the implant behind the nipple. Rather the male nipple is located at the bottom edge of the muscle/implant edge. It is not uncommon to see pectoral implants where the implant sticks out beyond the lateral muscle border, creating more of a flatter breast mound rather than a complete muscle augmentation.

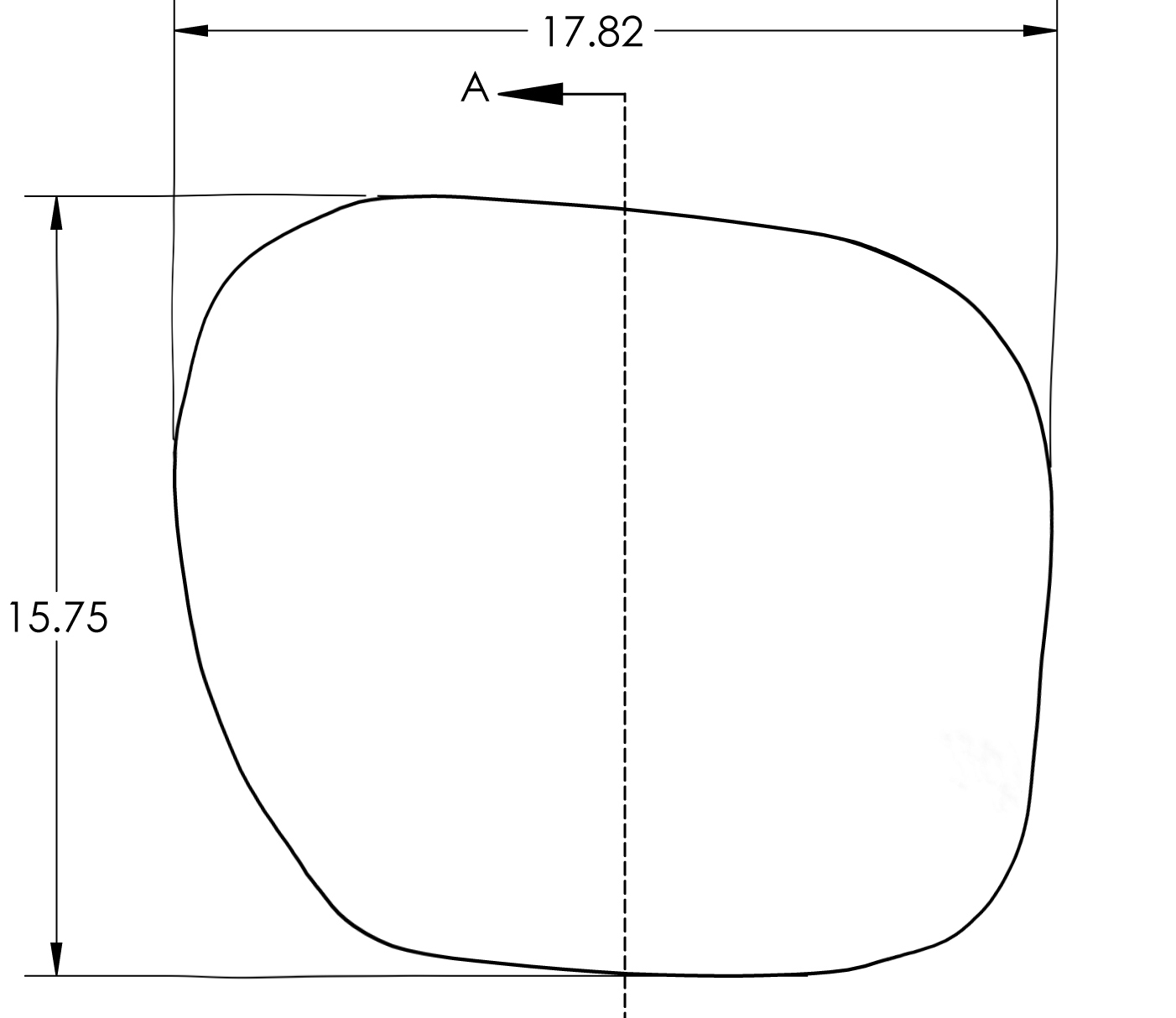 Pectoral implants come in several different shapes but they fundamentally come down to oval vs more of a rectangle. In looking at the shape of the pectoral muscle most men seek a more rectangular augmentation which augments the whole muscle. The lateral pectoral border is not straight but curved. A pure rectangular shape should only be used for the man who wants a straighter and not curved lateral pectoral margin. Preoperative measurements should be done from the sternal margin out to the lateral pectoral border and the implant width chosen on that basis. Some pectoral implants have tails that go up to the edge of the lateral pectoral border of the axilla at the thickest part of the muscle. Whether this has a useful augmentation effect canoe debated but at the least it may help with implant orientation.
Pectoral implants come in several different shapes but they fundamentally come down to oval vs more of a rectangle. In looking at the shape of the pectoral muscle most men seek a more rectangular augmentation which augments the whole muscle. The lateral pectoral border is not straight but curved. A pure rectangular shape should only be used for the man who wants a straighter and not curved lateral pectoral margin. Preoperative measurements should be done from the sternal margin out to the lateral pectoral border and the implant width chosen on that basis. Some pectoral implants have tails that go up to the edge of the lateral pectoral border of the axilla at the thickest part of the muscle. Whether this has a useful augmentation effect canoe debated but at the least it may help with implant orientation.
Male pectoral implants can be just as successful as that of breast implants in women. Technically it can be more successful long-term since pectoral implants have no risk of rupture.deflation and ever needing replaced due to device failure. Following several basic principles of the incision, pocket creation and implant selection will avoid most common pectoral implant problems.
Dr. Barry Eppley
Indianapolis, Indiana