

 Botulinum toxin, most commonly known as Botox, has a wide range of uses of which not all are FDA-approved. One of these yet-to-be-approved but growing uses is in injection into the masseter muscle. Being the second largest muscle in the face (the temporalis is the largest), it also differs from the other facial muscles being injected since it is not a muscle of facial expression. It is a masticatory or jaw moving and chewing muscle. There are two primary reasons to use Botox injections into the masseter muscle, one being for aesthetic facial contouring and the other for the relief of jaw-related facial pain.
Botulinum toxin, most commonly known as Botox, has a wide range of uses of which not all are FDA-approved. One of these yet-to-be-approved but growing uses is in injection into the masseter muscle. Being the second largest muscle in the face (the temporalis is the largest), it also differs from the other facial muscles being injected since it is not a muscle of facial expression. It is a masticatory or jaw moving and chewing muscle. There are two primary reasons to use Botox injections into the masseter muscle, one being for aesthetic facial contouring and the other for the relief of jaw-related facial pain.
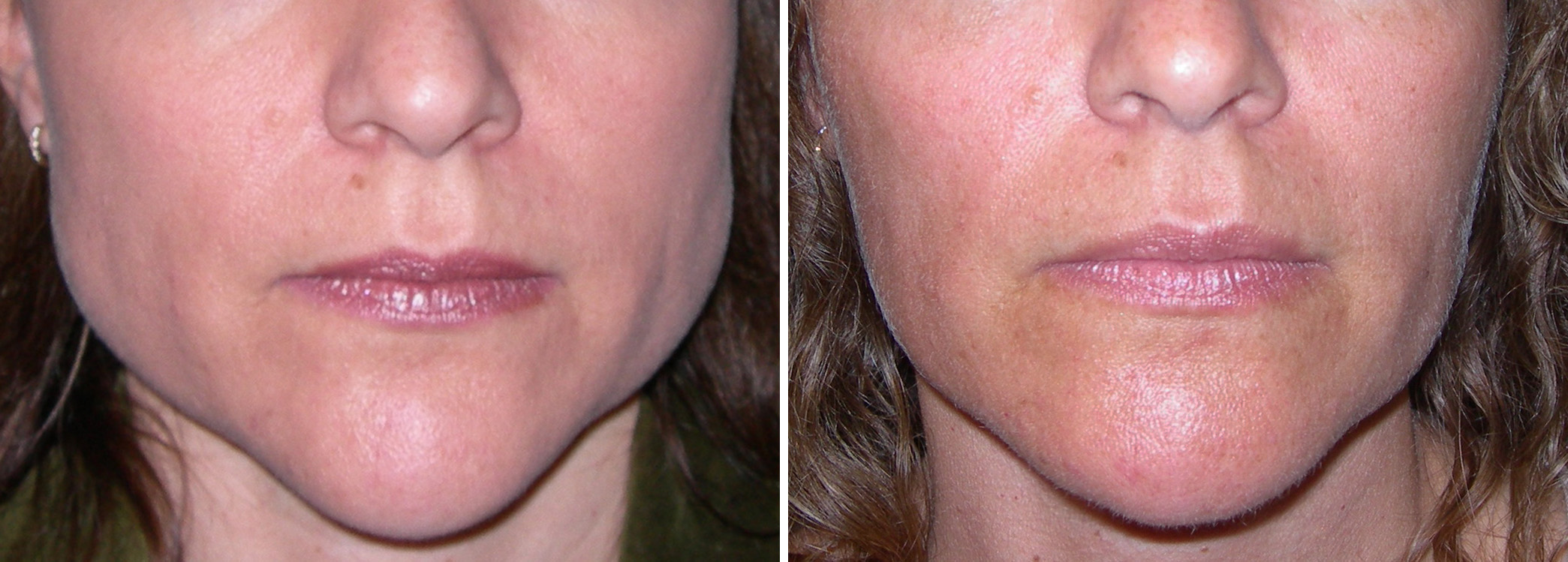
Some patients with a very square face may have a significantmasseter muscle thickening or hypertrophy. The contribution of the masseter muscle thickness to the width of the face can be determined by having the patient bite down and looking and feeling the size of the muscle. Extreme flaring or bulging is a sign of a significant contribution to facial width. Masseter muscle reduction is a commonly requested procedure in Asian ethnicities, particularly Korean, due to their inherently wider facial shapes. Compared to surgical thinning of the masseter muscle which is a very traumatic procedure with a long recovery, Botox injections offer an equal result without any of the surgical side effects.
 Botox injections can shrink the masseter muscle very effectively but is highly dose and location dependent. A dose of 25 units per masseter muscle is a good starting point and always produces a result. Less of a dose may also work but it is based on the size of the target. The equivalent dose of Dysport would be 50 to 75 units. It is important to inject only into the prominent bulges of the muscle on biting down. Placing it into normal muscle is a waste of injectate and may risk a cheek indentation, particularly at the anterior border of the muscle. It is also important to not inject above an imaginary line that runs between the tragus of the ear and the corner of the mouth. Going above that line places the buccal branch of the facial nerve at risk for months of temporary paralysis of the upper lip.
Botox injections can shrink the masseter muscle very effectively but is highly dose and location dependent. A dose of 25 units per masseter muscle is a good starting point and always produces a result. Less of a dose may also work but it is based on the size of the target. The equivalent dose of Dysport would be 50 to 75 units. It is important to inject only into the prominent bulges of the muscle on biting down. Placing it into normal muscle is a waste of injectate and may risk a cheek indentation, particularly at the anterior border of the muscle. It is also important to not inject above an imaginary line that runs between the tragus of the ear and the corner of the mouth. Going above that line places the buccal branch of the facial nerve at risk for months of temporary paralysis of the upper lip.
For this cosmetic facial shaping use, the effect becomes apparent relatively quickly within a month or two. The effects will last about 6 months and repeat injections are needed to sustain the narrowing effect. It is unknown if there is a point when the effect is sustained without further treatments.
For those who suffer from facial pain due to bruxism or excessive clenching, Botox has a similar beneficial effect. It not only stops the amount of muscle spasm and clenching but it can also cause a muscle thinning effect. The injection technique is the same but slightly higher doses may be needed. While I always start with 25 units of Botox per side, optimal pain relief may require a higher dose. But start at 25 units and see what happens. Also, because the temporalis muscle may be a contributor to the clenching, injection into it with 10 units may be needed. The injection point is determined by where the patient points to a temporalis location, but it is often into the muscle just above the zygomatic arch at the anterior edge of the hairline. The duration of these masseter muscle injections approximates that of its upper facial cosmetic effects of around 4 months. Despite this shorter duration, the pain relief can be dramatic.
Dr. Barry Eppley
Indianapolis, Indiana