

Excessive brow bone protrusion, known as brow bone hypertrophy, is a well recognized phenomenon that is due to over pneumatization of the frontal sinus. While many people think that it is due to excessive bone growth, it is actually due to an over enlargement of the frontal sinus air cavity. This pushes out the air cells making the brow bone and lower forehead look like a ‘bubble’ is sticking out from the bone. It can occur in different patterns from a large horizontally protruding brow bone across the top of the eyes to extensions up further up and out from the brow bone. It is a forehead growth pattern that is seen almost exclusively in men.
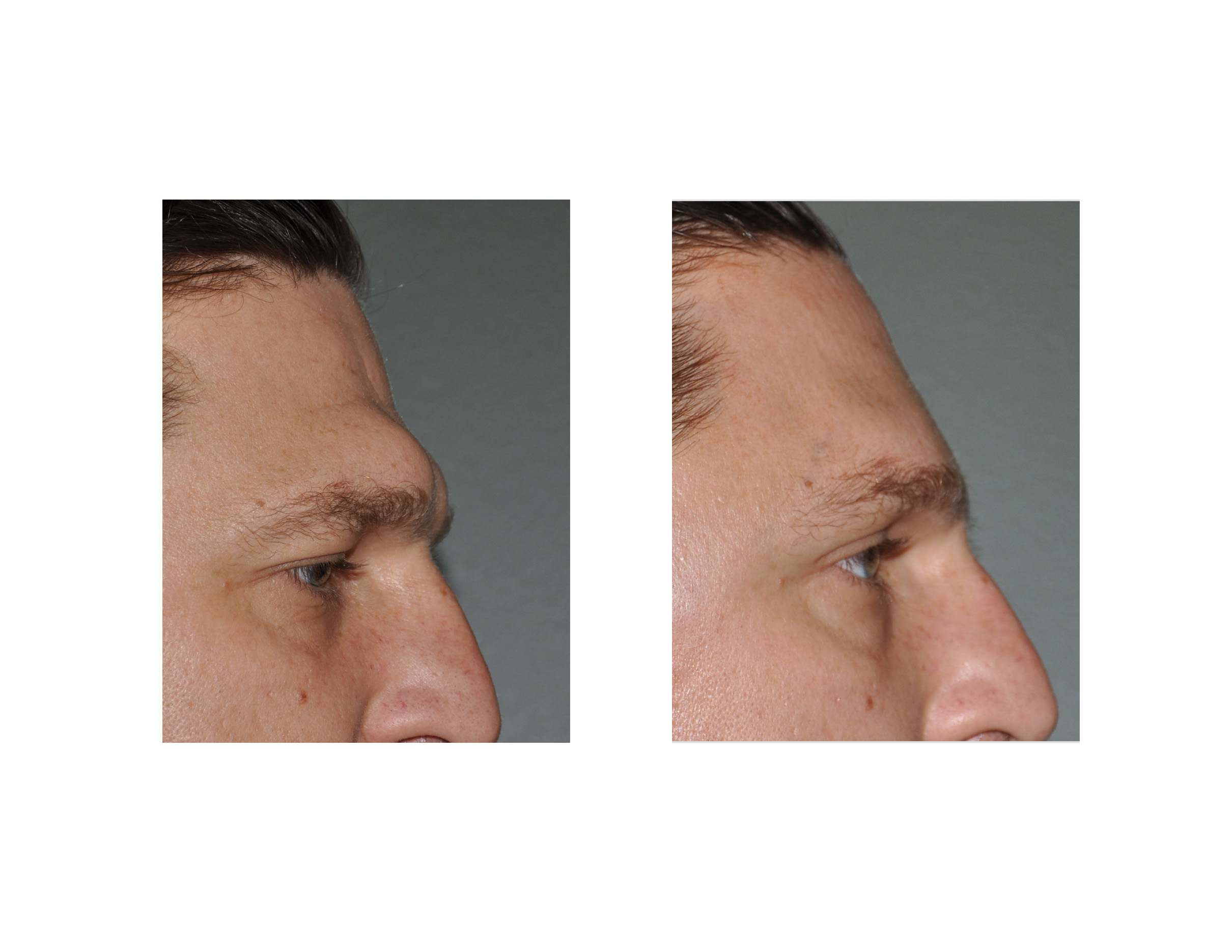 The approaches to brow bone reduction are fundamentally two-fold, either burr the brow bone down or remove the outer cortex of the brow bone and completely reshape and re-insert it. In men with any significant amount of brow bone protrusion, the bone removal/reshaping approach (osteoplastic flap method) is the one that is most effective and will make the greatest difference. The success of bone burring is limited by the thickness of the outer bony cortex of the frontal sinus which is usually only a few millimeters.
The approaches to brow bone reduction are fundamentally two-fold, either burr the brow bone down or remove the outer cortex of the brow bone and completely reshape and re-insert it. In men with any significant amount of brow bone protrusion, the bone removal/reshaping approach (osteoplastic flap method) is the one that is most effective and will make the greatest difference. The success of bone burring is limited by the thickness of the outer bony cortex of the frontal sinus which is usually only a few millimeters.
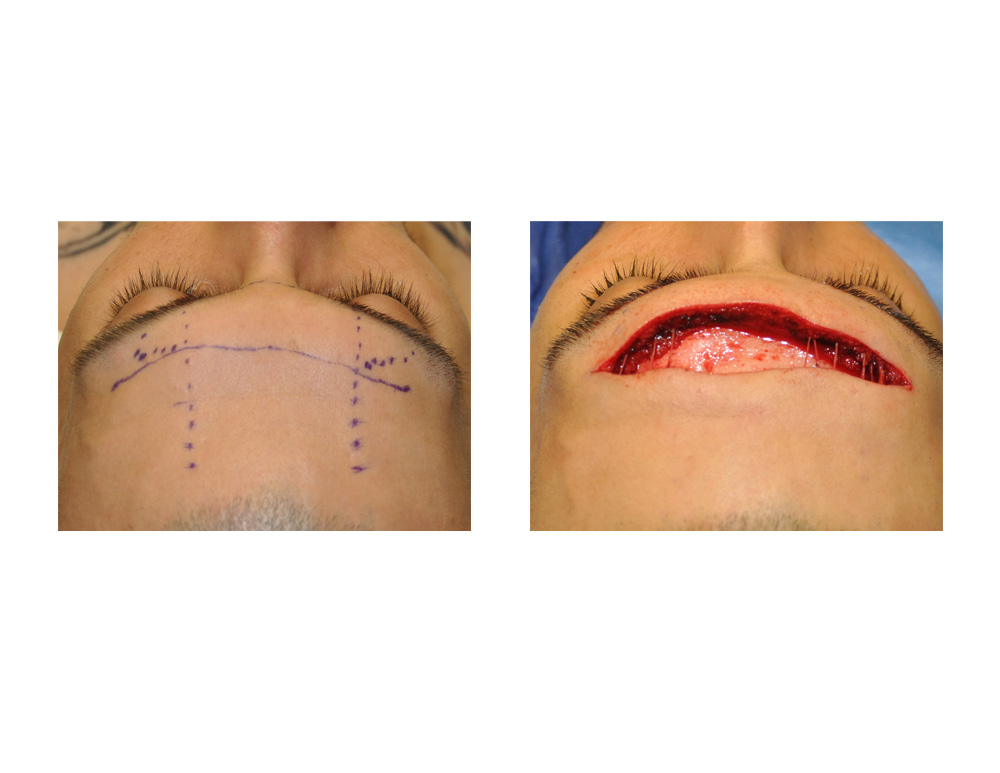
The real issue in male brow bone reduction surgery is not the method to do it but the surgical access. Because any form of effective brow bone reduction requires open exposure an incisional access is needed. Typically this is done from a coronal or scalp incision and if one has a good hair density this would be the preferred placement of the incision. But for men with thin hair or who shave their head a coronal incision may not be aesthetically acceptable. This leaves the alternative option of a forehead incision through an existing horizontal wrinkle line.
A mid-forehead approach provides direct access to the brow bones and involves far less tissue dissection than that of the more traditional coronal scalp incision. It requires one to have an existing horizontal wrinkle line which is preferable to get the best scar outcome. But besides the scar the other aesthetic trade-off would be a high likelihood of permanent forehead and anterior scalp numbness. The mid-forehead horizontal incision will directly transect the branches of the supraorbital and supratrochelar nerves that run vertically up the forehead from their exit from the bony foramen usually located on the bottom of the brow bones. While this does not affect movement of the forehead since these are sensory nerves, permanent numbness could be a bothersome long-term issue.

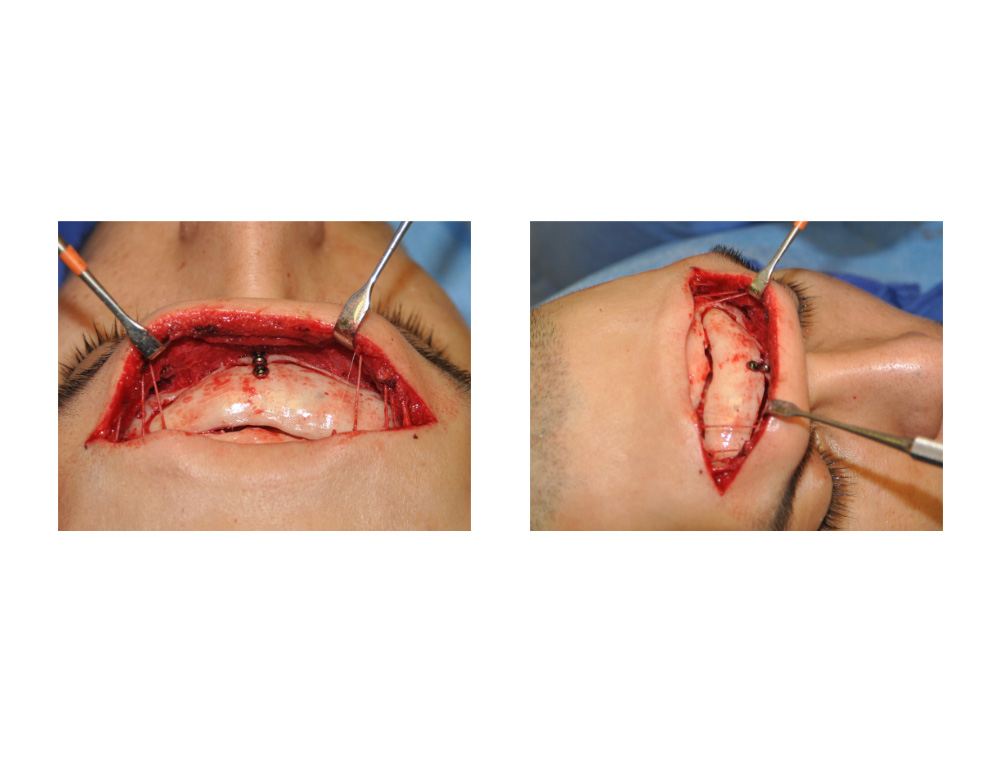 A nerve sparing technique can be used with the horizontal forehead incisional approach to the brow bones. After the skin incisions the vertical nerve branches are dissected out and spared. The brow bone surgery is then done by working underneath them. The brow bone flap is removed, reshaped, resinserted and then rigidly fixed, all while working in and around the spared nerve fibers. The incision is closed in layers with care taken to not inadvertently entrap the nerve branches in the sutures.
A nerve sparing technique can be used with the horizontal forehead incisional approach to the brow bones. After the skin incisions the vertical nerve branches are dissected out and spared. The brow bone surgery is then done by working underneath them. The brow bone flap is removed, reshaped, resinserted and then rigidly fixed, all while working in and around the spared nerve fibers. The incision is closed in layers with care taken to not inadvertently entrap the nerve branches in the sutures.
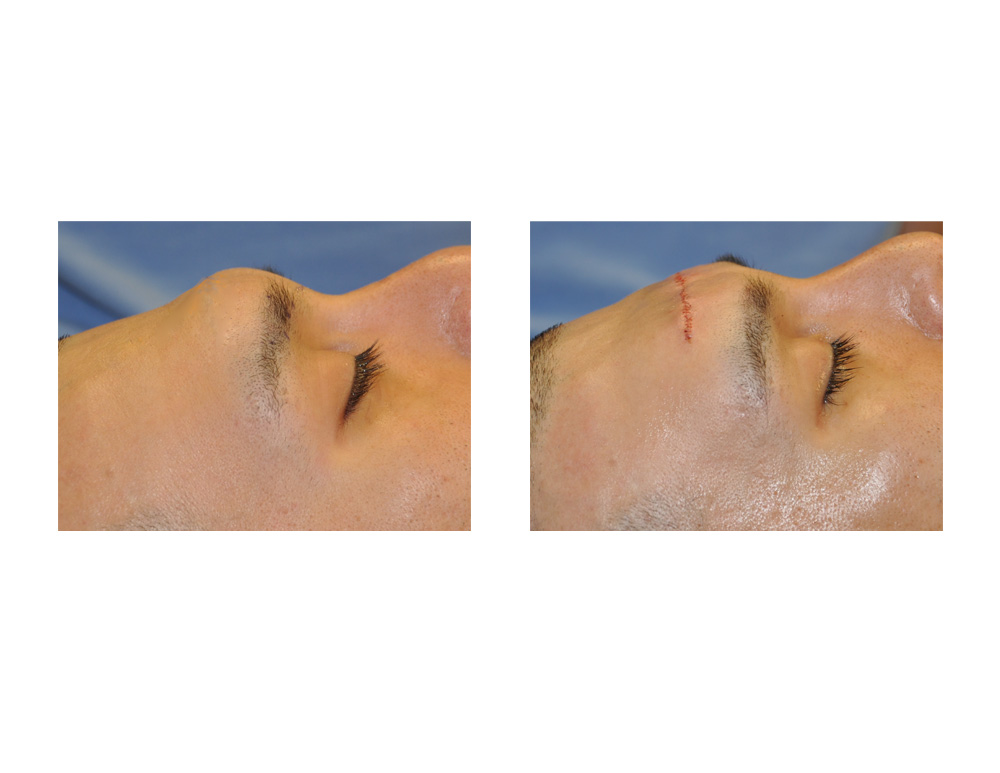 A nerve sparing forehead incision brow bone reduction technique can produce a very successful setback of the brow bones. While the spared nerve branches do get stretched a little during the procedure they are more likely to allow a return of forehead feeling that if they were completely transected.
A nerve sparing forehead incision brow bone reduction technique can produce a very successful setback of the brow bones. While the spared nerve branches do get stretched a little during the procedure they are more likely to allow a return of forehead feeling that if they were completely transected.
Dr. Barry Eppley
Indianapolis, Indiana