

Background: Few women have perfectly symmetric breasts. While most women would acknowledge that anatomic fact, most women would prefer to not undergo an aesthetic procedure where their natural asymmetry becomes magnified. But this is exactly what can happen in breast augmentation surgery. Two symmetrically shaped and sized implants will merely enlarge what exists before surgery and some asymmetries can become even more apparent.
The two breast asymmetries where this can happen are horizontally oriented ones, the inframammary folds and the nipple-areolar complexes. The nipples are not directly affected by underlying volume expansion so it is easy to see that a preoperative difference in the horizontal level of the nipples can be even bigger as the mound size increases. Differences in the level of the inframammary folds is often a reflection of differences in mound size. Keeping the current fold levels will affect how the breast mounds will look as they become bigger also.
In small breasts it is important to look for subtle differences in them before implant surgery. It may be small and often unrecognized by the patient only to become readily identified after surgery when they spend a lot more time looking at their own breasts. Considerations of a superior areolar lift (crescent lift) and lowering the higher inframammary fold are options to discuss before surgery in women with breast asymmetry before their augmentation surgery.
Case Study: This young female presented for breast augmentation. The left breast was seen to be smaller with a higher inframammary fold and a lower nipple position. The differences for each one was less than 1 cm. It was decided to concurrently lift the lower nipple but keep the inframamamry folds at the same level…with the understanding that perfect breast symmetry would not occur after surgery.
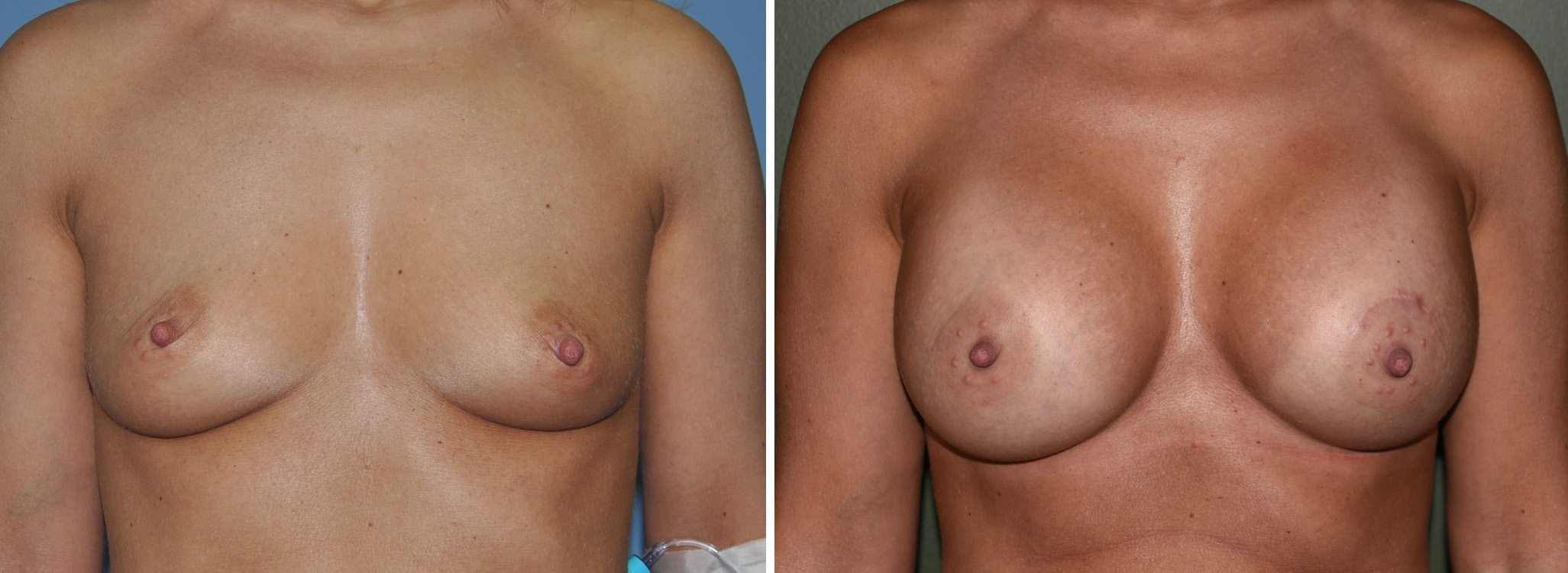
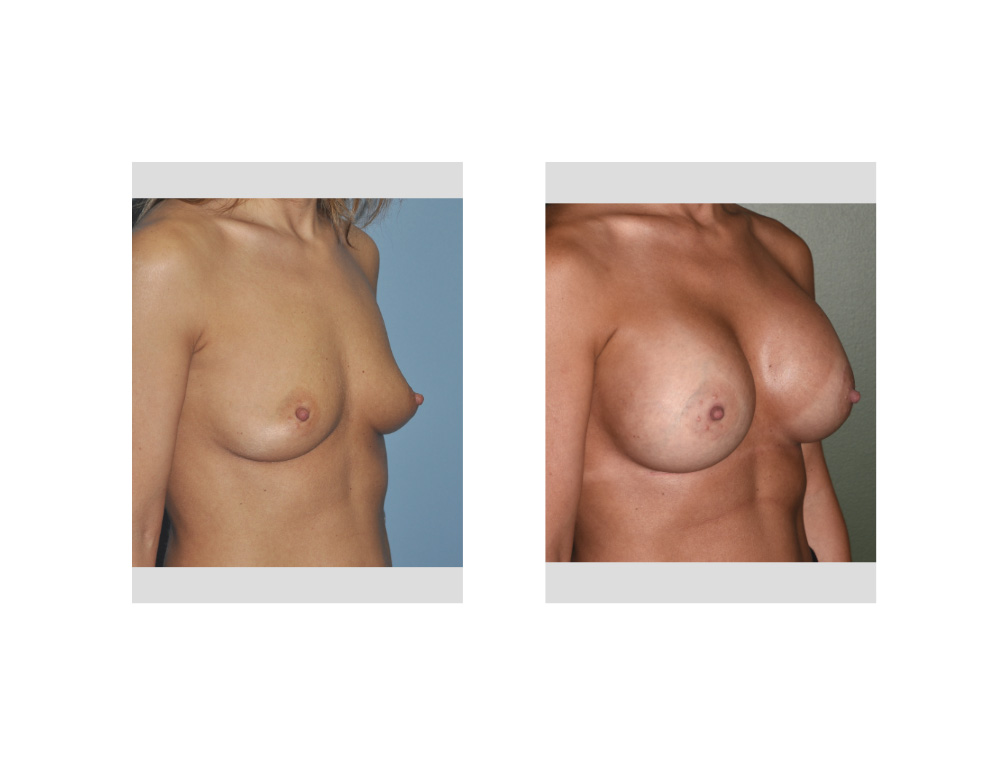 Under general anesthesia she had 350cc cohesive silicone gel implants placed through inframammary fold inciseons. A superior crescent lift of 8mms was done on the left nipple. After surgery her nipples were at the same horizontal level and slight differences in the breast mounds remained.
Under general anesthesia she had 350cc cohesive silicone gel implants placed through inframammary fold inciseons. A superior crescent lift of 8mms was done on the left nipple. After surgery her nipples were at the same horizontal level and slight differences in the breast mounds remained.
Recognizing subtle breast asymmetries before implant surgery provides the opportunity for considering management strategies at the same time. While nipple lifts can always be done after surgery under local anesthesia, adjustments of the inframammary fold is not quite so easily done.
Highlights:
1) Breast asymmetry is common in women receiving implant augmentation which can affect the aesthetic outcome of the procedure..
2) Different inframammary fold and horizontal nipple positions are the common asymmetries seen, some of which can be improved with ancillary procedures.
3) Changing the inframammary fold level and raising the position of the superior areolar border are two helpful asymmetry procedures in breast augmentation.
Dr. Barry Eppley
Indianapolis, Indiana