

Background: Modifications of the ribcage can be done for a variety of body contouring reasons. Most commonly posterior rib removals are done for anatomic waistline narrowing. By removing the ends of ribs 10, 11 and 12, the width of the waistline can be narrowed in width by removing the ‘obstructions’. This is ribcage modification done for a transverse or width body improvement.
But above the level of the free floating ribs, the ribcage is a circumferential structure. Underneath the breasts/chest is the bottom end of the ribcage known as the subcostal region. It consists mainly of ribs 7, 8 and 9. In some patients these bottom ribs may stick out or protrude creating an unaesthetic bulge.
Anterior rib removals, like that of posterior rib removals, can be done for aesthetic trunk modification. The most direct approach to them is through a small subcostal incision over their lower portion. By removing or shaving the lower subcostal ribs the protrusion of the ribcage can be reduced. Such modifications can also increase the vertical length of the waistline by increasing the distance between the lower end of the ribcage and the hips.
Case Study: This young transgender female was bothered by a subcostal protrusion of her ribs. She would rather have a small subcostal scar than ribs that stick out.
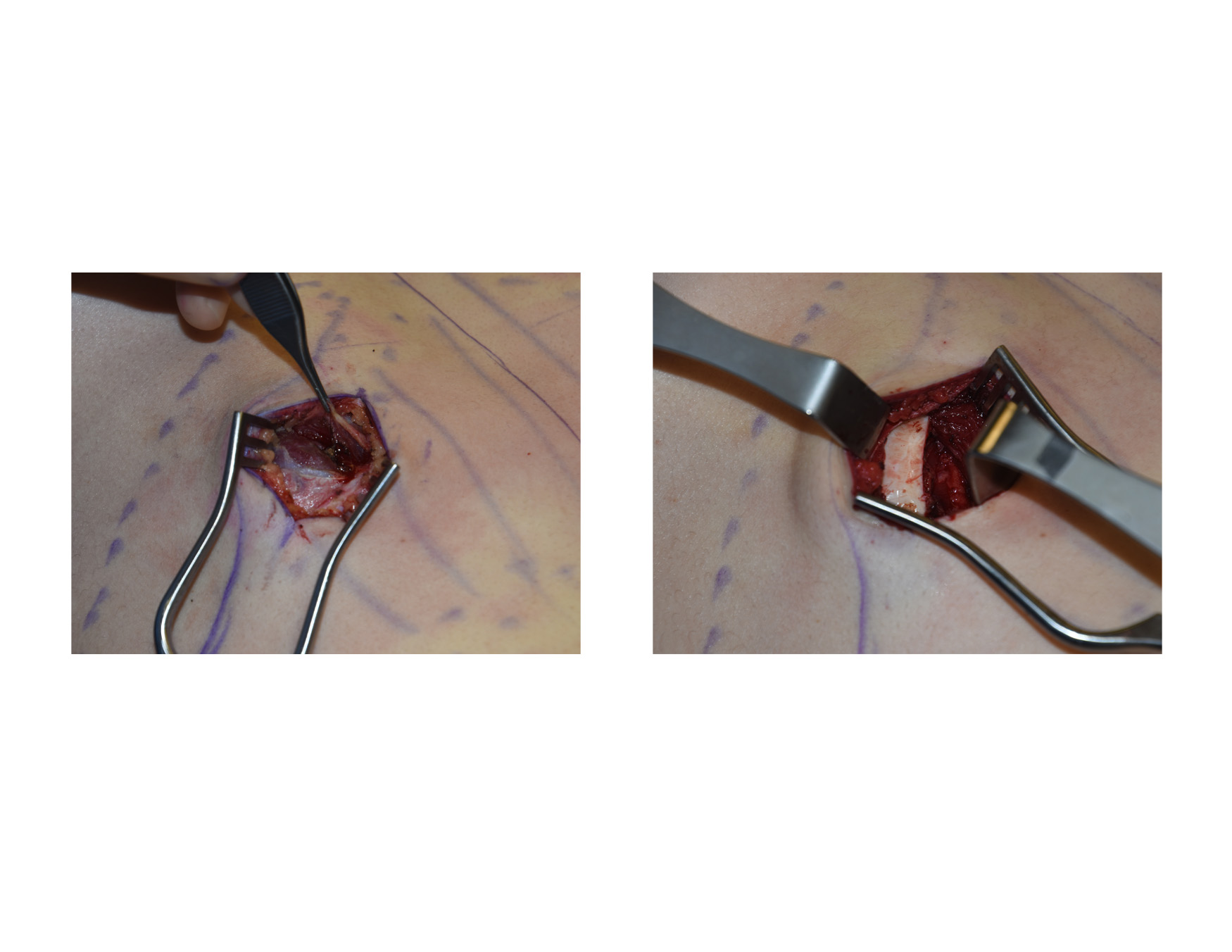
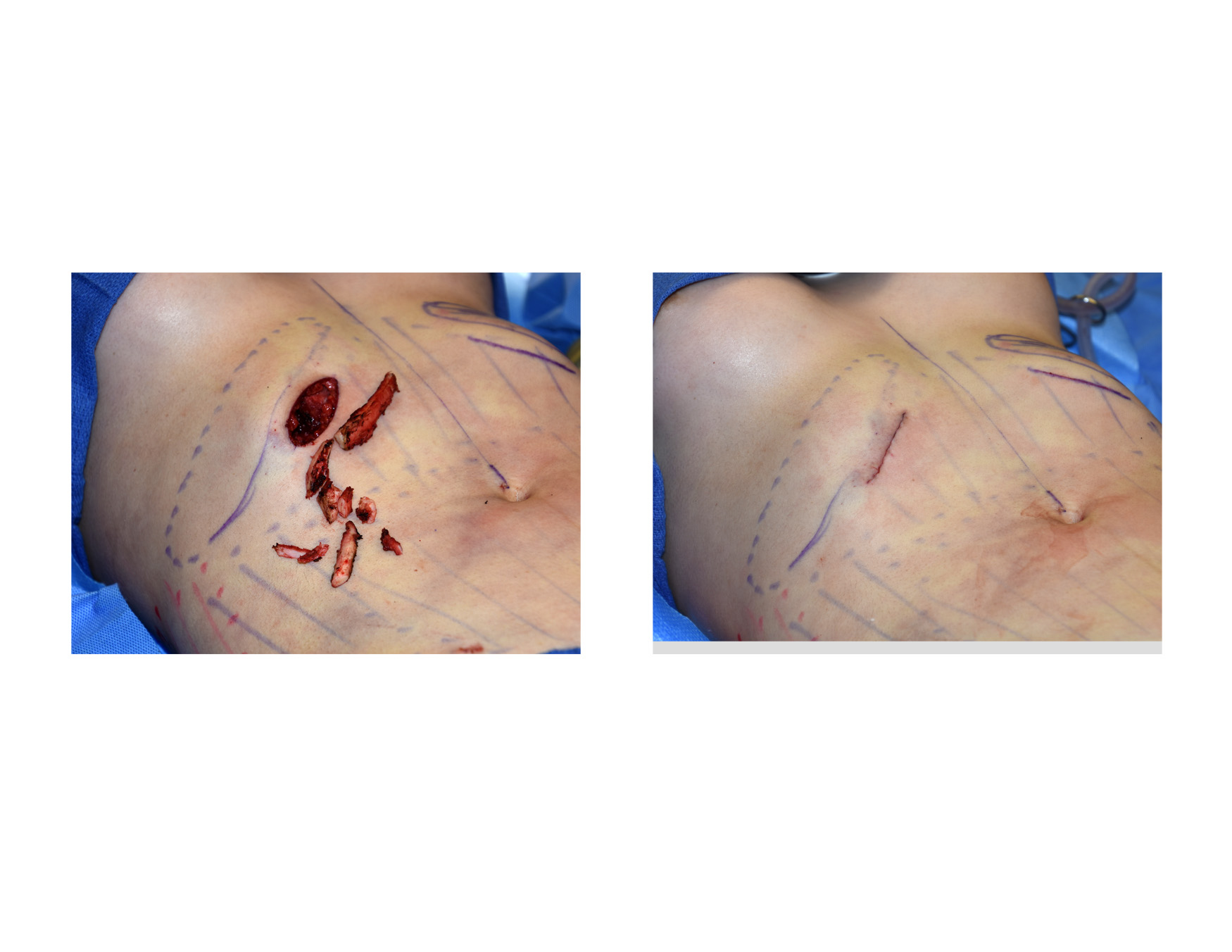 Under general anesthesia and through a 4.5cm central subcostal incision, the lower ribs were accessed by splitting the overlying rectus muscle. The cartilaginous portions of ribs 8 and 9 were removed from the sternum out laterally to their bony junction. Rib #7 was significantly reduced by shaving its lower edge.
Under general anesthesia and through a 4.5cm central subcostal incision, the lower ribs were accessed by splitting the overlying rectus muscle. The cartilaginous portions of ribs 8 and 9 were removed from the sternum out laterally to their bony junction. Rib #7 was significantly reduced by shaving its lower edge.
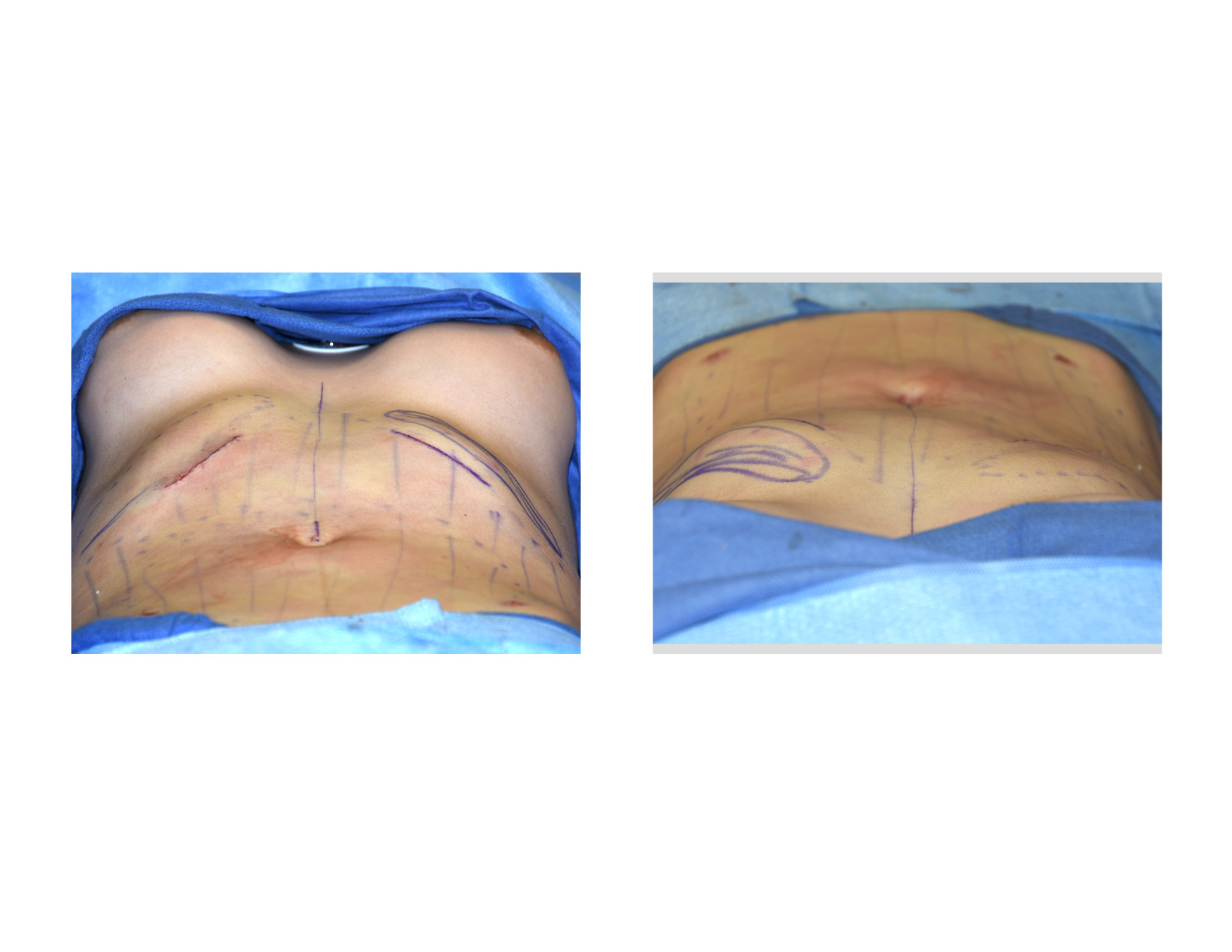 The change in the lower ribcage protrusion was immediately apparent during surgery when the treated side was compared to the yet to be treated side. The flow from the breasts into the abdomen was smooth and more concave.
The change in the lower ribcage protrusion was immediately apparent during surgery when the treated side was compared to the yet to be treated side. The flow from the breasts into the abdomen was smooth and more concave.
 Anterior rib protrusions are more of a concern for women as they produce a noticeable bulge at the upper abdomen. Such a hard prominence also vertically shortens the waistline between the lower end of the ribcage and the hips.
Anterior rib protrusions are more of a concern for women as they produce a noticeable bulge at the upper abdomen. Such a hard prominence also vertically shortens the waistline between the lower end of the ribcage and the hips.
Rib removals can be done as either a posterior, anterior or combined technique. These modifications are done at the lower end of the front and back part of the ribcage for different body contouring effects. Because they are at the bottom of the ribcage such rib removals are associated with a very low risk of any significant problems. The lower end of the pleura of the lungs is close by and knowledge of its location is paramount for safe rib removal surgery.
Highlights:
1) Vertical waistline lengthening involves anterior rib removals.
2) Anterior rib removals are also useful to reduce ribs that stick out at the bottom of the ribcage.
3) Anterior rib removals are done through a small subcostal incision or can be done through a full tummy tuck approach.
Dr. Barry Eppley
Indianapolis, Indiana