

Plastic SurgeryBackground: The need for augmentation of the nose can be due to congenital, traumatic or iatrogenic saddle nose deformities or for elective ethnic rhinoplasty surgery. Ethnic rhinoplasty indications are usually for the Asian or African-American patient in my practice and are dorsal line augmentations that usually involve the tip as well. The debate is such nasal augmentation is always one of using the patient’s own tissues (cartilage) or that of the a nasal implant.
The debate of an autogenous vs. alloplastic rhinoplasty is not new and the advantages and disadvantages of both are well known. An implant rhinoplasty simplifies the operation, provides and assured shape and saves the patients any extranasal graft harvest site. But it is an implant and with that comes an increased risk of infection and the potential for ong-term tissue thinning and exposure. Conversely the need for a substantative cartilage graft requires a rib graft harvest with an uncomfortable donor site and scar and the potential for warping of the dorsal graft. But a rib graft has a very minimal risk of infection and no danger of long-term tissue thinning or extrusion.
Nasal implants often have a bad reputation in the mind. of many plastic surgeons. There are certainly easily findable major complications from them that can be located on the internet. But like all surgical implants of any type, how and when they are used plays a major role in their ultimate success and failure. Large nasal implants, dorsocolumellar implant styles that cross the tip area, and noses with thin tissues all increase the risk profile of what is really a subcutaneous synthetic implant.
Case Study: This 24 year Asian female was undergoing numerous facial reshaping procedures of which one was that of a rhinoplasty. She desired a higher bridge from the radix down to the tip. A nasal implant vs a rib graft was discussed thoroughly and she opted for the nasal implant.
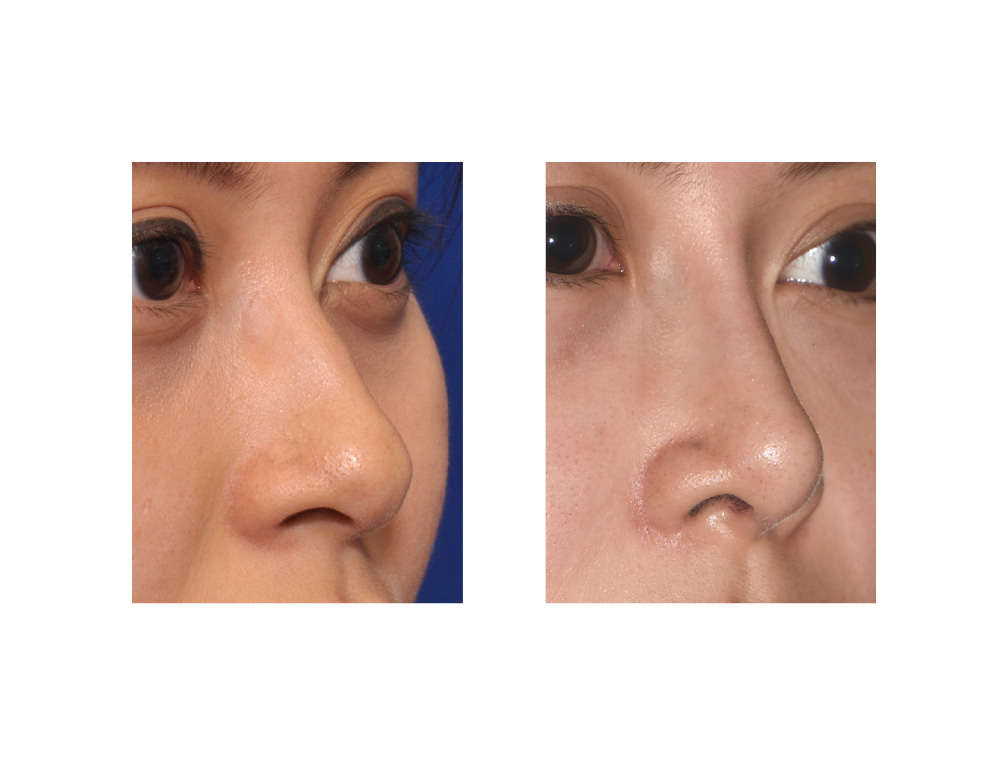
 Under general anesthesia she had an open rhinoplasty through which a silicone implant was used for the bridge and a septal cartilage graft for the tip. The bridge was built up with a medium Implantech dorsal nasal implant that had 3.5mms at the radix and 4mms at its lower end which was placed under the dome. The nasal tip had increased projection through a septal columellar strut graft and tip suturing techniques.
Under general anesthesia she had an open rhinoplasty through which a silicone implant was used for the bridge and a septal cartilage graft for the tip. The bridge was built up with a medium Implantech dorsal nasal implant that had 3.5mms at the radix and 4mms at its lower end which was placed under the dome. The nasal tip had increased projection through a septal columellar strut graft and tip suturing techniques.

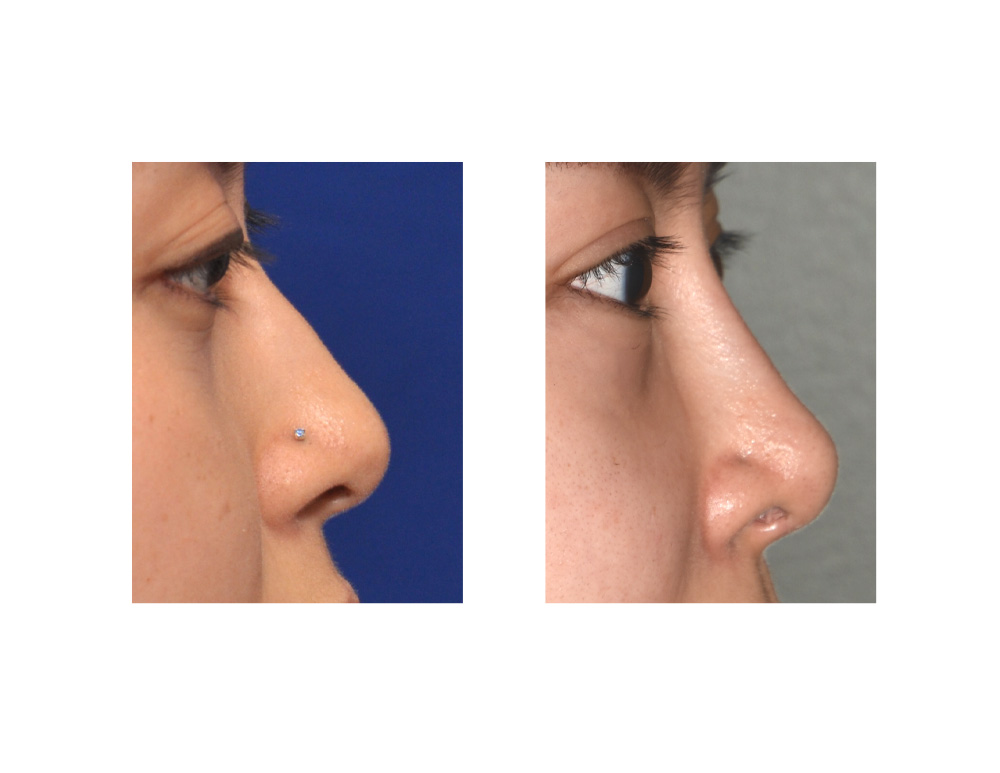 At six months after her implant rhinoplasty she had a nice straight nose with a higher dorsal projection. Smoothness and straightness of the dorsum are the aesthetic advantages offer by an implant. This style of dorsal nasal implant is fairly narrow in width and is best used in women and not men for this shape reason. A pencil thin nose in men is usually not an ideal nasal look.
At six months after her implant rhinoplasty she had a nice straight nose with a higher dorsal projection. Smoothness and straightness of the dorsum are the aesthetic advantages offer by an implant. This style of dorsal nasal implant is fairly narrow in width and is best used in women and not men for this shape reason. A pencil thin nose in men is usually not an ideal nasal look.
 Nasal implants can be used very successfully if they are not asked to do too much augmentation and in the carefully selected patient. Limiting the augmentation to the dorsum and not the nasal tip and avoiding excessively high amounts of augmentation will help diminish the risk of complications with their use to very low levels.
Nasal implants can be used very successfully if they are not asked to do too much augmentation and in the carefully selected patient. Limiting the augmentation to the dorsum and not the nasal tip and avoiding excessively high amounts of augmentation will help diminish the risk of complications with their use to very low levels.
Highlights:
- Nasal implants often have a bad reputation when their success is tied more to their use and the patient’s nasal augmentation needs
- Dorsal nasal implants have a high rate of success when the amount of augmentation needed is not excessive.
- Nasal implants avoid the need for a rib graft harvest and offer a more assured straight nose that permanently stays so.
Dr. Barry Eppley
Indianapolis, Indiana