

Background: Women that want breast augmentation present with a wide array of breast shapes and sizes. The post-pregnancy breast that has become deflated (lost volume) and has some sagging is one of the common ‘abnormal’ breast types seen. But even within this type of breast shape there are subtypes or different variations within this general category. The lean bodied female with thin skin and stretch marks is one of these subtypes that has essentially a loose deflated sac of skin that just hangs over the lower breast fold.
What makes this type of breast augmentation challenging is how to avoid the need for a breast lift. No woman really wants a breast lift and in cases of significant breast sagging it would be unavoidable. But it is the mild breast sagging cases that can pose a dilemma. It is the size of implant chosen that can determine how to manage the breast sagging. If a small breast implant size is used, then a vertical breast lift will be needed. If a moderate implant is placed, a periareolar or donut lift could be adequate. If a larger implant is used, then a superior nipple lift may be all that is needed.
The definition of what constitutes a small, medium and large breast implant will be different for each patient and it is open to interpretation. But that can be determined based on the patient’s natural breast base width and how the implant’s dimensions compare to it. Larger breast implants in women with thin breast tissues may risk loss of support and bottoming out later but can potentially avoid scars on the breast.
Case Study: This 40 year-old female wanted to reshape her breasts with a much bigger size as well as correct her sagging. She had a very thin body frame with small deflated breasts with thin skin and a narrow breast base width. (12 cms) While the potential need for a lift was discussed with her, she did not want any breast scars and opted for an implant size that was at the perimeter of her breast base width. The potential lower nipple position was felt to be better than any scars.
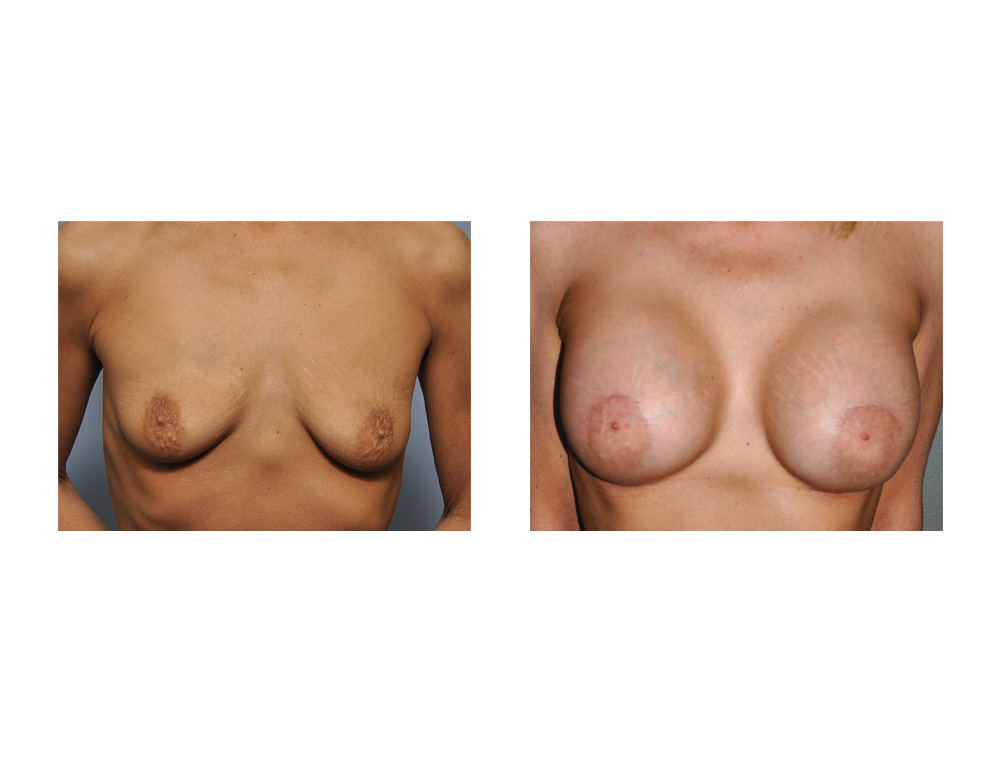
 Under general anesthesia, 450cc high profile silicone implants were placed through a lower breast fold incision. (the location of the incision was placed lower than her natural breast crease to accomodate the implant size and provide a bit of a ‘nipple lift’) After the placement of the implants, a superior crescent mastopexy (upper nipple lift) of 1 cm was done to help center the nipple on the new enlarged breast mounds.
Under general anesthesia, 450cc high profile silicone implants were placed through a lower breast fold incision. (the location of the incision was placed lower than her natural breast crease to accomodate the implant size and provide a bit of a ‘nipple lift’) After the placement of the implants, a superior crescent mastopexy (upper nipple lift) of 1 cm was done to help center the nipple on the new enlarged breast mounds.
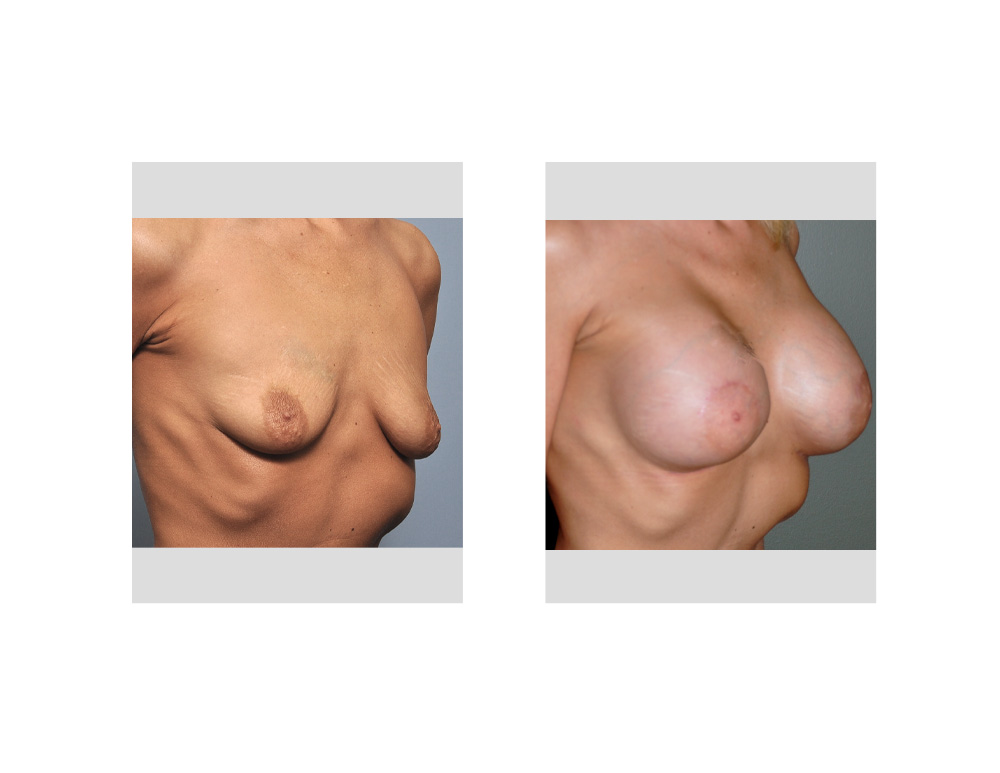
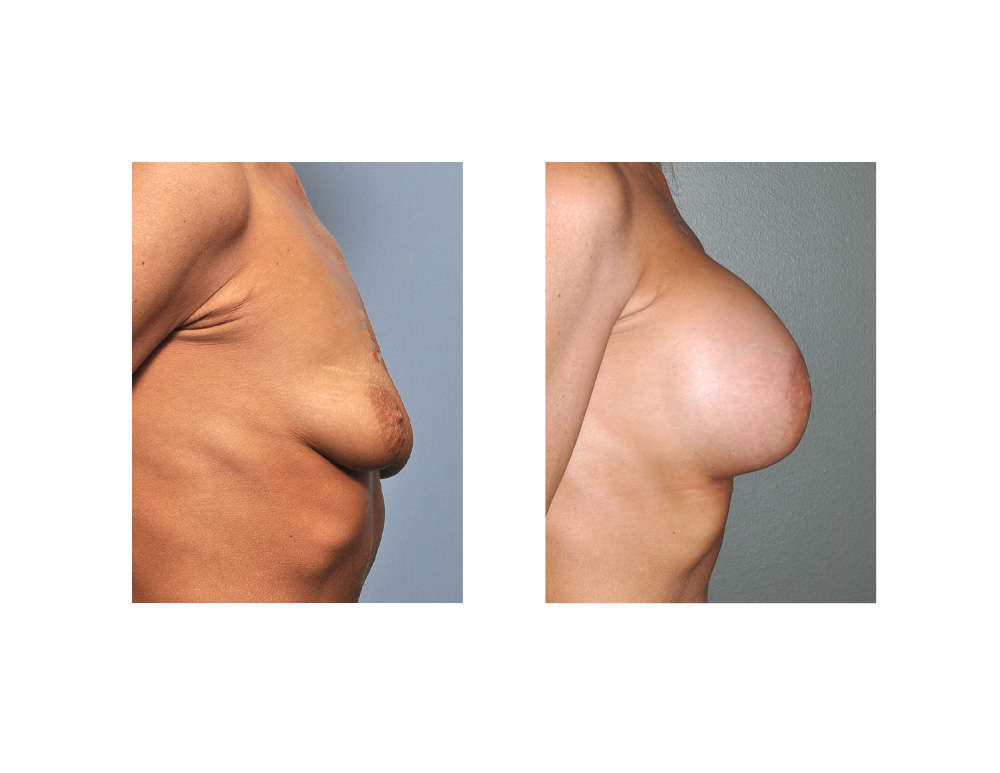 Avoiding a breast lift in a sagging breast is always challenging and can really only be accomplished in one with minimal to moderate sag. The slightly sagging breast with thin skin and little volume does get a bit of a lift with larger implants. The volume addition is particularly enhanced when the inframammary crease is lowered. (although this maneuver does increase the risk of bottoming out and the creation of a lower pole double bubble) It is usually necessary to add a superior nipple lift as part of the breast reshaping procedure to help center the nipple on the breast as best as possible. Even with the combined implant and nipple lift technique, some women may still have to accept a breast that is slightly ‘tilted’. (nipple slightly off center/low on the mound) But this trade-off may still be better than breast skin scars from a more formal lift.
Avoiding a breast lift in a sagging breast is always challenging and can really only be accomplished in one with minimal to moderate sag. The slightly sagging breast with thin skin and little volume does get a bit of a lift with larger implants. The volume addition is particularly enhanced when the inframammary crease is lowered. (although this maneuver does increase the risk of bottoming out and the creation of a lower pole double bubble) It is usually necessary to add a superior nipple lift as part of the breast reshaping procedure to help center the nipple on the breast as best as possible. Even with the combined implant and nipple lift technique, some women may still have to accept a breast that is slightly ‘tilted’. (nipple slightly off center/low on the mound) But this trade-off may still be better than breast skin scars from a more formal lift.
Case Highlights:
1) Deflated breasts that have thin skin and a moderate amount of sagging pose a challenge in breast augmentation surgery.
2) Vertical breast lift scars can be avoided in some mildly sagging breasts if large enough implants are used with an upper nipple lift.
3) There is a balance between the implant size used and the ability of the breast tissue/skin to support it.
Dr. Barry Eppley
Indianapolis, Indiana