

Background: The secondary management of cheek implants could include their removal or may involve their replacement which in my experience is more common. Typically in cheek implant replacement surgery the major focus is on what style and size of new cheek implant is needed as well its positioning on the zygomatic bone. Unlike chin implants cheek implants rarely affect the shape of the bone on which they are positioned. (passive bone remodeling) This is because the the overlying cheek soft tissues is not as tight as that of the chin pad.
Should one remodeling occur around cheek implants, and that always be at its front end, there is the potential risk of maxillary sinus exposure. Because the bone overlying the maxillary sinus between the anterior and posterior pillars is quite thin (2mms or less), any loss of bone could result in a full-thickness defect. While not an issue with in a healed cheek implant where it has occurred gradually, when a cheek implant is surgical exposed and a maxillary sinus wall defect is seen, this is an issue in its replacement due to the substantially increased risk of infection.
The question then becomes in cheek implant replacement with the surprising finding of exposure of the maxillary sinus is what to do. Should the new cheek implants not be placed and done later hoping the bone defect has healed or should the sinus defect be somehow closed and the new cheek implants put in immediately? Placing the cheek implants and ignoring the sinus exposure is not an option.
Case Study: This female had a history of Medpor cheek implants that were placed 11 years previously. She never really liked the result and wanted substantially increased fullness in the ‘apple cheek’ area. (anterior cheeks)
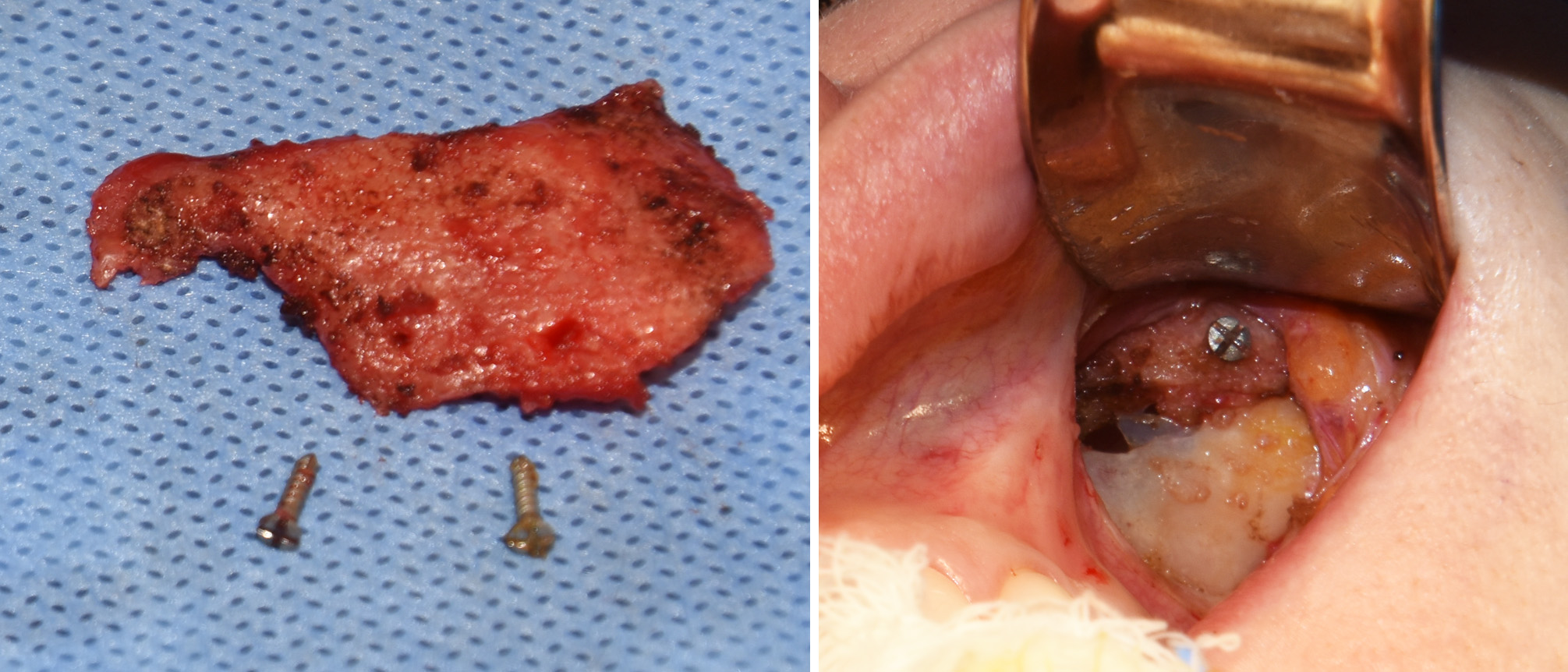
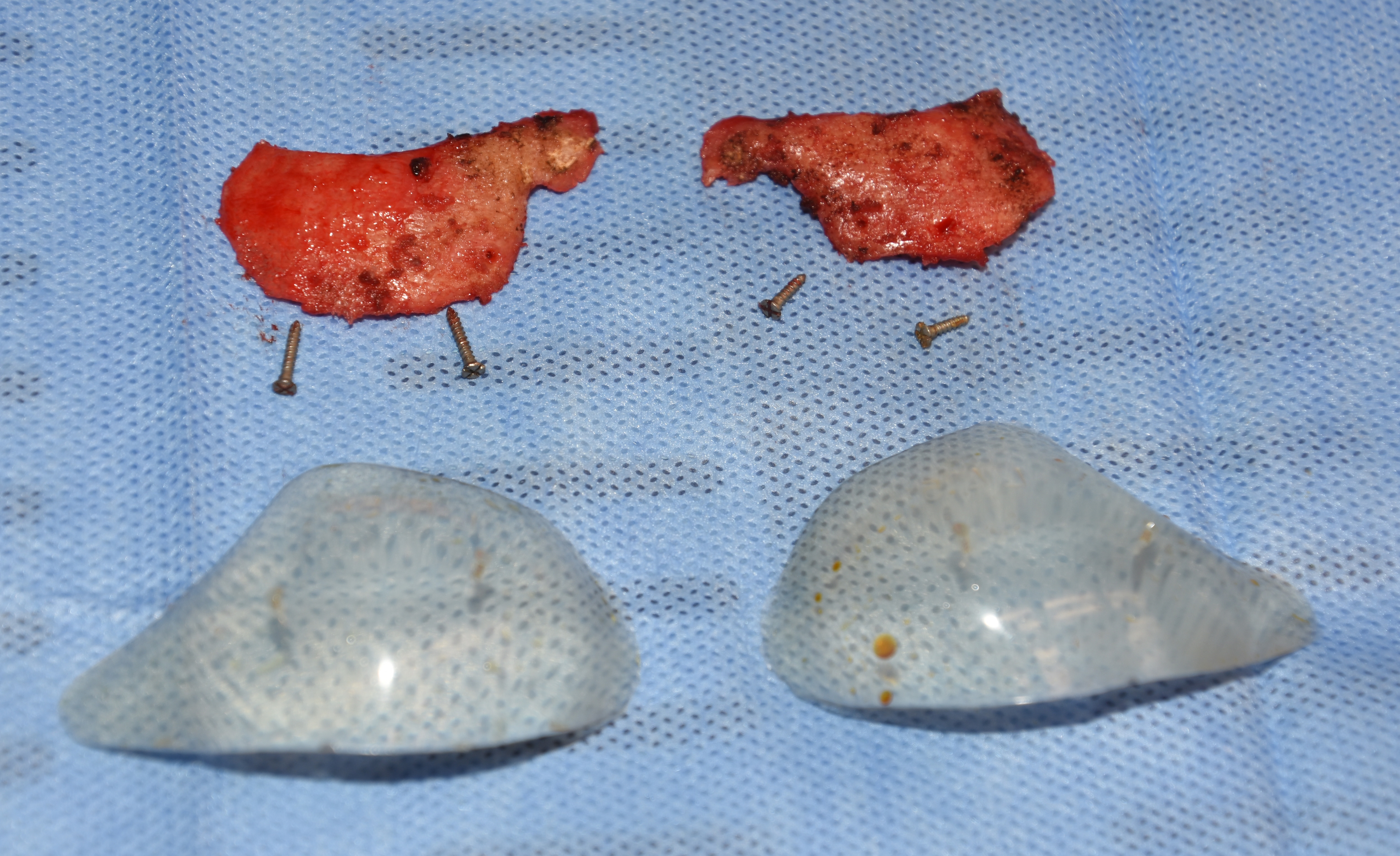 Under general anesthesia her previous cheek implants were exposed through a high maxillary vestibular incision. On the right side the cheek implant and. screws appeared as would be expected and were removed. On the left side, hwoever, a large maxillary sinus defect was found on the inferior aspect of the implant which was revealed to be bigger when the implant was removed.
Under general anesthesia her previous cheek implants were exposed through a high maxillary vestibular incision. On the right side the cheek implant and. screws appeared as would be expected and were removed. On the left side, hwoever, a large maxillary sinus defect was found on the inferior aspect of the implant which was revealed to be bigger when the implant was removed.
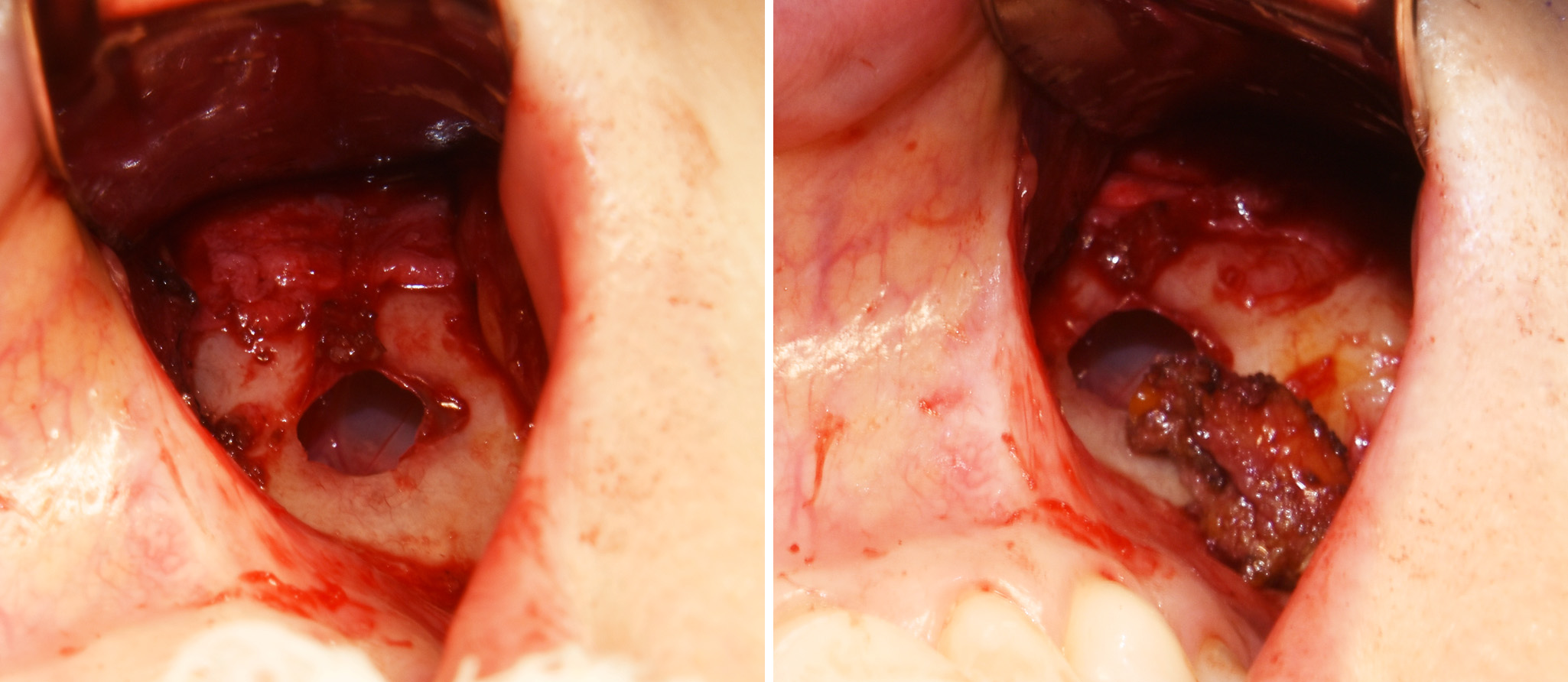
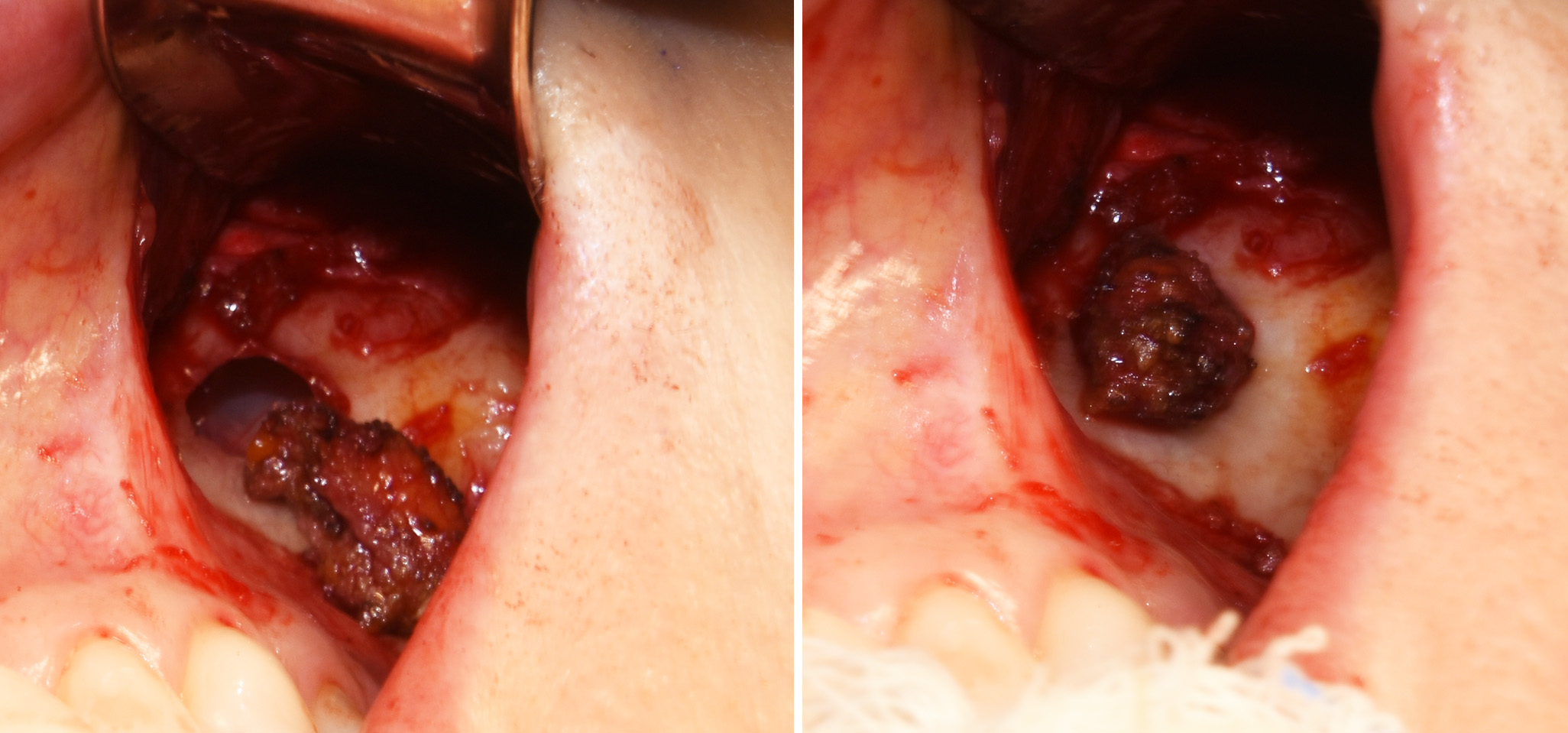 It was elected to proceed with the new cheek implants and cover the defect with a soft tissue graft/plug. She had a concurrent submentoplasty performed from which muscle and fat has been removed. This was used to place into the defect as a plug and the cheek implant was placed over it and secured with a screw.
It was elected to proceed with the new cheek implants and cover the defect with a soft tissue graft/plug. She had a concurrent submentoplasty performed from which muscle and fat has been removed. This was used to place into the defect as a plug and the cheek implant was placed over it and secured with a screw.
Defects of the maxillary sinus wall in an adult of any size will not spontaneously heal with restoration of an intact bony wall unless they are bone grafted. Thus delaying the cheek implant replacement and coming back in later would just re-expose the maxillary bone defect and be presented with the same problem. While bone grafting is always the most assured method of closing a maxillary sinus wall defect, in the unprepared aesthetic patient an autologous soft tissue graft is a reasonable alternative.
Highlights:
1) The removal of cheek implants that are positioned over the maxillary sinus may rarely cause an opening into the maxillary sinus.
2) If cheek implants are going to put back with a maxillary sinus exposure, the opening will need to closed preferably with a tissue graft.
3) The risk of infection is higher with cheek implant replacements when a maxillary sinus opening has been encountered.
Dr. Barry Eppley
Indianapolis, Indiana