

Background: Repair of a primary cleft lip deformity is one of the common pediatric plastic surgery procedures performed in infants. Usually done around three to four months of age, its repair is usually done by the rotation-advancement technique. This well established cleft lip repair procedure works by derotating the shortened medial lip element and bringing in the lateral lip element in its wake. Once in alignment the lip vermilion is then debulked and put together for a smoother and more uniform red part of the lip.
But despite how good a cleft lip repair may look at 6 months or one year of life, the effects of growth and scarring/wound contracture are often not kind. Over time many well-executed cleft lip repairs will change in appearance. The most common changes are shortening of the philtral length, notching of the vermilion lower lip edge and mismatching of the vermilion-cutaneous border at the Cupid’s bow area. As a result the need for secondary cleft lip revisions is the norm rather than the exception.
While there are numerous detailed techniques in cleft lip revision, one of the major ones used is the correction of a notched vermilion and to improve its projection/fullness. Realignment of the vermilion and mucosal V-Y advancements are useful secondary vermilion enhancement methods. One very effective method for improving vermilion full ness with a scar revision/realignment is a fat graft. Fat grafts not only bring in volume but healthy tissue as well.
Case Study: This 16 year-old female teenager was born with a right complete cleft lip and palate deformity. She had primary cleft lp and palate repairs as well as a secondary alveolar bone graft. As a teenager her initial cleft lip repair showed vertical philtral length shortening, an inverted V notch at the lower edge of the upper lip and lack of adequate projection/protrusion.

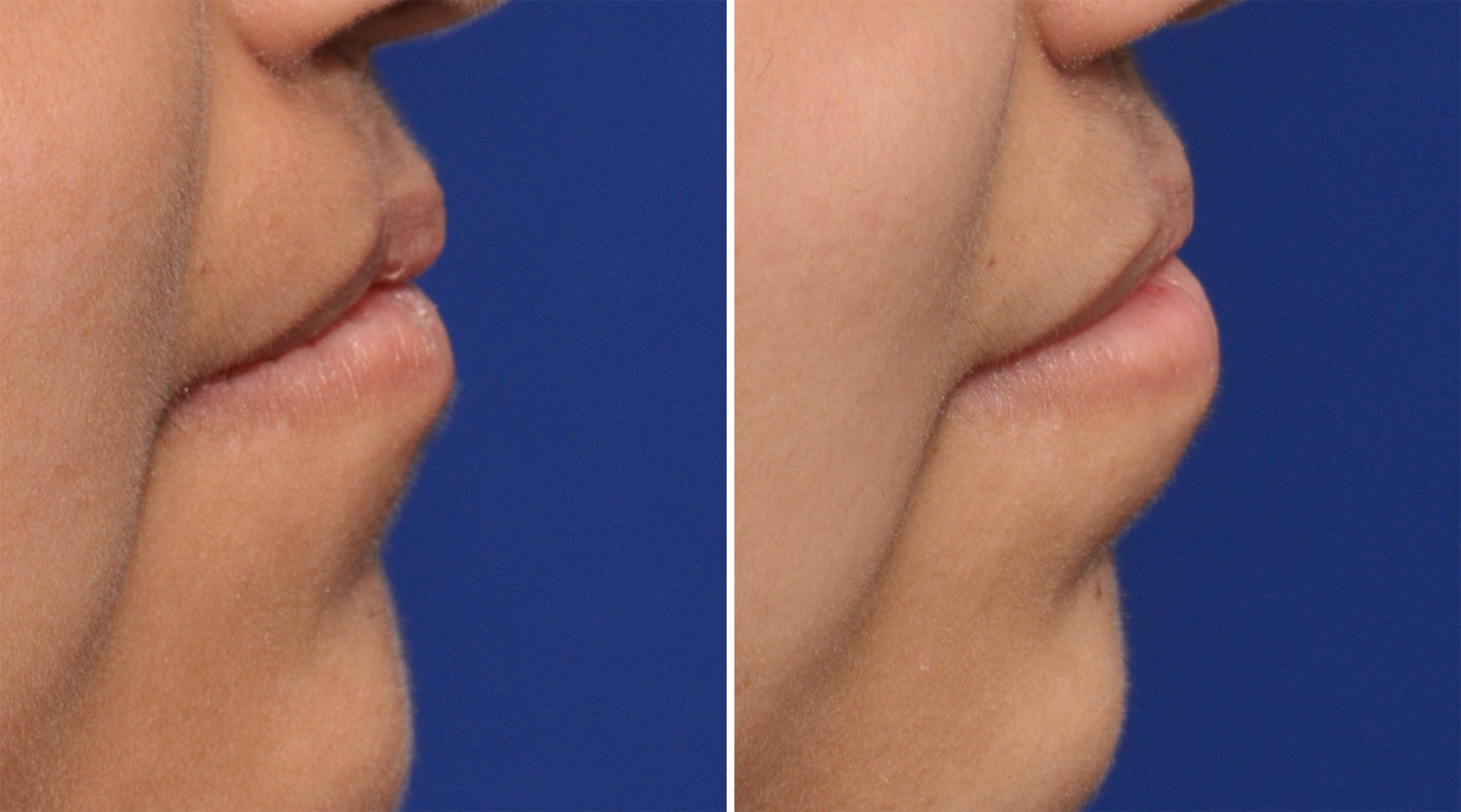 Under general anesthesia a V-Y mucosal advancement was done, rolling out the lip mucosa to help correct the inverted V notch deformity. To prevent its contraction with healing and to help add some lip volume a free fat graft was placed prior to its closure. The fat graft was harvested from the opposite buccal fat pad through an intraoral incision. Only a small piece of the buccal fat pad was needed. (much less than even a subtotal buccal lipectomy.
Under general anesthesia a V-Y mucosal advancement was done, rolling out the lip mucosa to help correct the inverted V notch deformity. To prevent its contraction with healing and to help add some lip volume a free fat graft was placed prior to its closure. The fat graft was harvested from the opposite buccal fat pad through an intraoral incision. Only a small piece of the buccal fat pad was needed. (much less than even a subtotal buccal lipectomy.
Many cleft lip revisions have a need for increased volume. Autologous fat is a logical soft tissue graft that can be incorporated into many cleft lip revisions. The buccal fad pad is both a regionally convenient and hardy fat source which can be harvested without scarring. The volume removed is minimal but still should be taken from the non-cleated side of the face since the buccal fat pad on the cleft is already slightly smaller in most cases.
Highlights:
- Very few primary cleft lip repairs ever do not need a secondary revision.
- One of the most common secondary cleft lip issues is a lack of vermilion volume.
- One source of adding additional volume is with the use of free fat grafts, specifically that from the buccal fat pad.
Dr. Barry Eppley
Indianapolis, Indiana