

Background: Fractures to the nose most commonly result in nasal deviations as the direction of the force usually comes from the side. (e.g.,fists) But direct trauma to the nose results in impaction injuries which push the nose inward resulting in loss of bridge height and a collapsed nasal appearance.
The most severe type of nasal impaction injury comes from high velocity forces such as motor vehicle accidents. This not only pushes the nose in but the extension of the fracture lines and bony displacement extends to the medial orbits as well. This results in not only the nose being pushed inward but the attachments of the eyelids (medial canthi) end up being displaced laterally. These traumatic nose and eye changes create what is known as a traumatic hypertelorism effect. (technically pseudohypertelorism) This can be very hard to correct during the initial fracture repair and often requires secondary surgery for a more complete correction.
 Case Study: This teenage female was involved in an ATV accident where she sustained blunt trauma to her face at the frontonasal area by striking a tree. She sustained a severe naso-ethmoid fracture pattern as well as other facial bone fractures. She underwent primary facial fractures repair any another facility, part of which was done through a coronal scalp incision. When seen six months after her initial injury and repair, she had a telecanthic appearance with indentation of her nasal bridge.
Case Study: This teenage female was involved in an ATV accident where she sustained blunt trauma to her face at the frontonasal area by striking a tree. She sustained a severe naso-ethmoid fracture pattern as well as other facial bone fractures. She underwent primary facial fractures repair any another facility, part of which was done through a coronal scalp incision. When seen six months after her initial injury and repair, she had a telecanthic appearance with indentation of her nasal bridge.
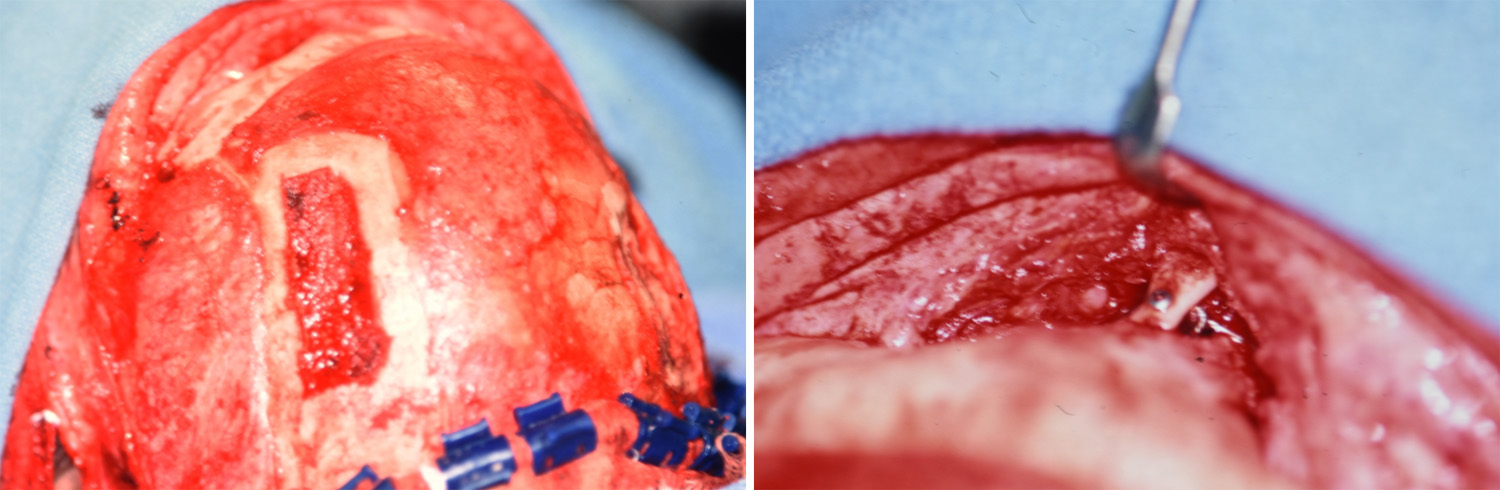 Under general anesthesia, her original coronal scalp incision was opened and the scalp reflected down to the nasofrontal junction. A split-thickness outer table cranial bone graft was harvested from the left posterior forehead region which had a minimal curvature to it. The graft was shaped to fit the length of the nose and inserted into a nasal pocket and secured at its superior end with a 2.0 molar screw. The graft donor site was reconstructed to contour with hydroxyapatite cement. Medial canthoplasties using 3o0 gauge wires was also done, passing it under the cranial bone graft.
Under general anesthesia, her original coronal scalp incision was opened and the scalp reflected down to the nasofrontal junction. A split-thickness outer table cranial bone graft was harvested from the left posterior forehead region which had a minimal curvature to it. The graft was shaped to fit the length of the nose and inserted into a nasal pocket and secured at its superior end with a 2.0 molar screw. The graft donor site was reconstructed to contour with hydroxyapatite cement. Medial canthoplasties using 3o0 gauge wires was also done, passing it under the cranial bone graft.

 At five years after her secondary nasal reconstruction, her dorsal nasal height remained stable and straight. The bone graft showed no signs of resorption.
At five years after her secondary nasal reconstruction, her dorsal nasal height remained stable and straight. The bone graft showed no signs of resorption.
 Her eyes appears closer together which was probably as much the result of a heightened nasal bridge as the medial canthoplasties.
Her eyes appears closer together which was probably as much the result of a heightened nasal bridge as the medial canthoplasties.
Highlights:
- One graft option in nasal reconstruction is cranial bone due to its anatomic proximity.
- Cranial bone grafts to the nose usually undergo minimal long-term resorption
- Through a coronal scalp incision, a cranial bone graft to the nose can be done with medial canthoplasties in the treatment of traumatic hypertelorism.
Dr. Barry Eppley
Indianapolis, Indiana