

Background: Jaw asymmetry is one of the most common forms of perceived facial asymmetry. Whether it is localized to the chin or extends back along the jawline to involve the two jaw angles as well affects the magnitude of the deformity. The long length of the body of the mandible and the size of the jaw angles, compared to that of the much smaller chin, usually makes the facial asymmetry more obvious.
Patients undergoing orthognathic surgery frequently have bony asymmetry. When recognized before surgery it is usually built into the surgical plan and some adjustment accounted for by the osteotomy cuts. But such preoperative jawline asymmetries often persist after surgery and others can inadvertently be created by the surgery, particularly when sagittal split osteotomies of the ramus (SSRO) are done. How the bone cuts are made on each side, how the segments are put back together once the occlusion is set in the oral splint and the potential for some postoperative bony resorption due to the tissue stripped off of the bone all create the potential for the postsurgical occurrence or the magnification of presurgical asymmetry.
The treatment of jawline asymmetry, if augmentation is the corrective approach (which it almost always is), is best done with a custom jawline implant. The only relevant preoperative question is whether one or both sides should be treated.
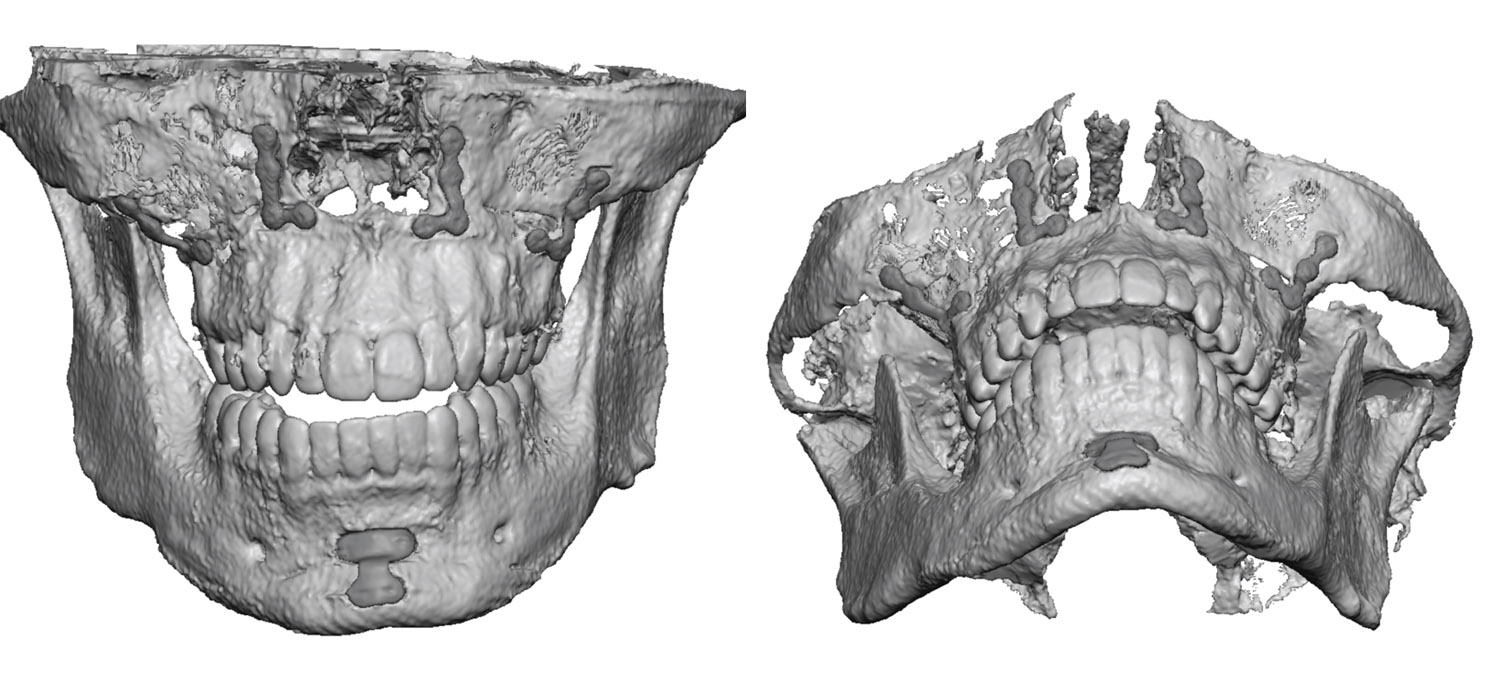 Case Study: This young male had a prior bimaxillary orthognathic surgical procedure. He acknowledged that facial asymmetry existed prior and was unclear if it was the same or worse than before that surgery. A 3D CT scan showed a tilt to the face with the left side being smaller than that of the right. From the chin back to the jaw angle the left side ws vertically shorter and less wide. His interest was to correct the left-sided facial asymmetry as well as enhance the overall jawline any a modest amount.
Case Study: This young male had a prior bimaxillary orthognathic surgical procedure. He acknowledged that facial asymmetry existed prior and was unclear if it was the same or worse than before that surgery. A 3D CT scan showed a tilt to the face with the left side being smaller than that of the right. From the chin back to the jaw angle the left side ws vertically shorter and less wide. His interest was to correct the left-sided facial asymmetry as well as enhance the overall jawline any a modest amount.
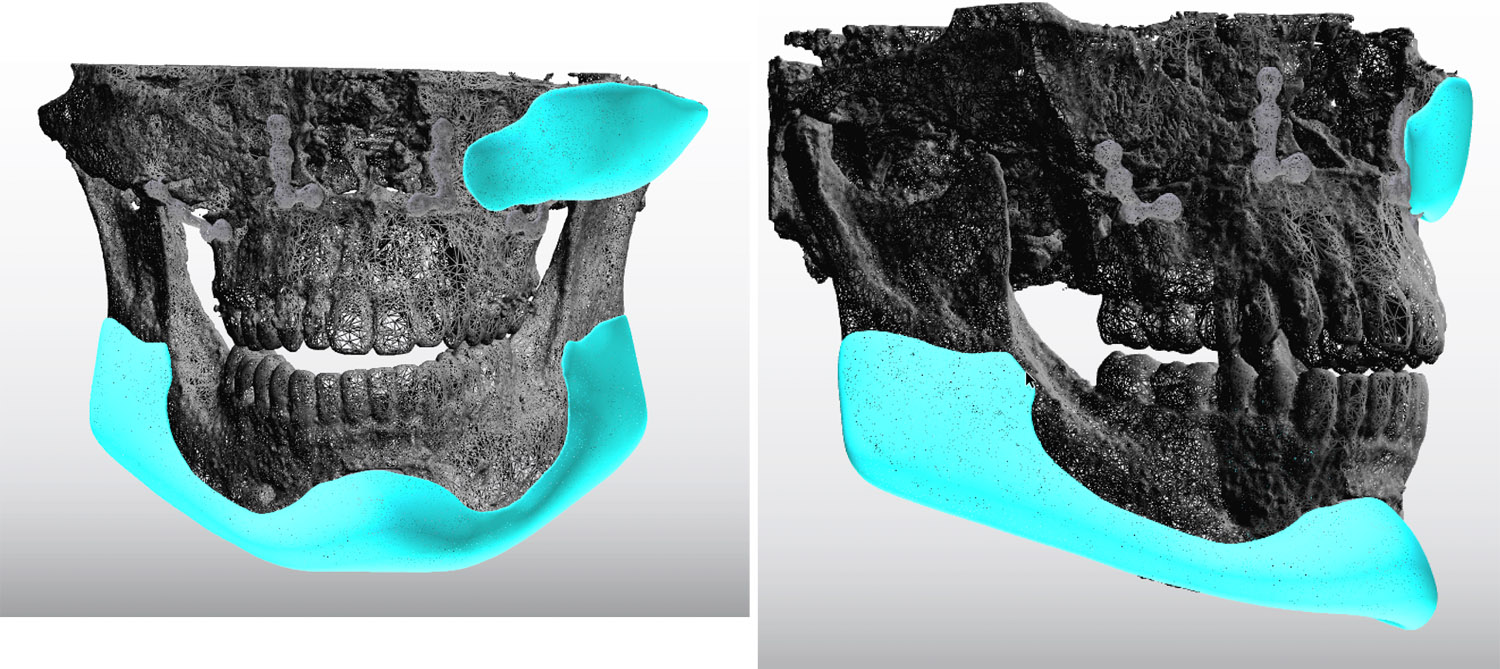
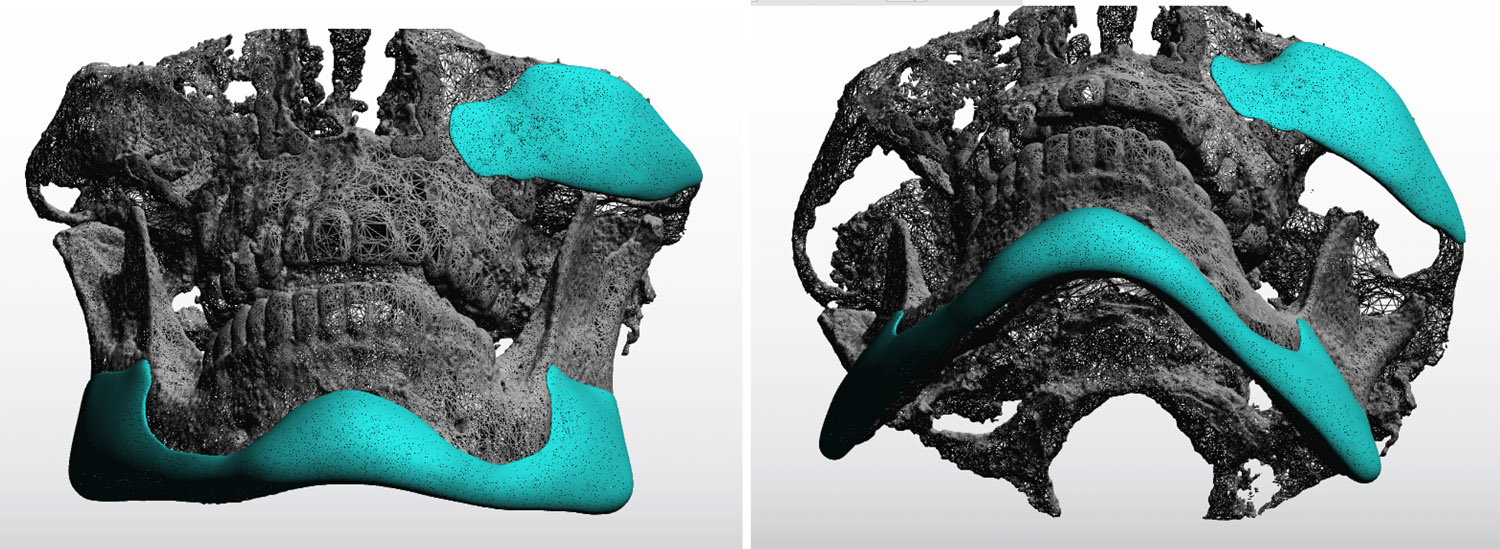
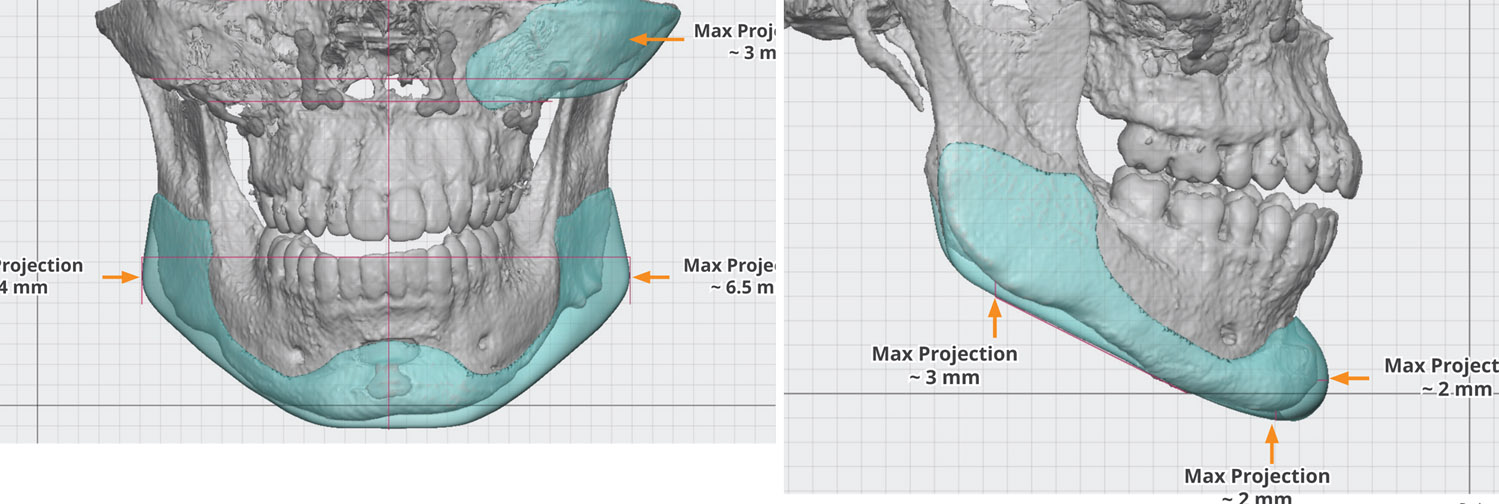 From this scan a two implant approach was designed to augment the whole jawline, factoring in the smaller left side, as well as a small cheek implant to augment the more subtle left cheek flatness. Both implants were relatively small as the goal was not to create some dramatic facial change.
From this scan a two implant approach was designed to augment the whole jawline, factoring in the smaller left side, as well as a small cheek implant to augment the more subtle left cheek flatness. Both implants were relatively small as the goal was not to create some dramatic facial change.
 Under general anesthesia the custom jawline implant was placed through a completely intraoral approach using three internal incisions. These were used to tread the jawline implant into place. The left cheek implant was placed through a standard intraoral upper lip vestibular incision.
Under general anesthesia the custom jawline implant was placed through a completely intraoral approach using three internal incisions. These were used to tread the jawline implant into place. The left cheek implant was placed through a standard intraoral upper lip vestibular incision.
The complete correction of any facial asymmetry is difficult and a perfect result should probably be considered unrealistic. There is always the variable of the surgical placement of the implants whose perfect positioning is never assured. (it is not as easy as the implat designs make it appear) But custom designed facial implants adds one symmetric variable to an otherwise asymmetric situation and gives the best chance to improve the facial asymmetry as much as possible.
Highlights:
1) Jawline asymmetry is not uncommon after orthographic surgery and may or may reflect presurgical asymmetry.
2) A 3D CT facial scan is the best method to accurately diagnosis the location and extent of the jaw asymmetry.
3) A custom jawline implant can be designed to treat the entire jawline and is always best to create an overall jaw enhancement as well.
Dr. Barry Eppley
Indianapolis, Indiana