

Background: Undereye hollows is a very common aesthetic issue for both young and older patients alike. In older patients it is often a function of soft tissue atrophy that exposes the underlying orbital bone, creating a skeletonized appearance. Conversely in the younger patient it is more a function of a hard tissue deficiency rather than a soft tissue atrophy situation.
A bony or skeletal underdevelopment issue around the lower eye is known as a negative orbital vector. This is where bony support under the eye us deficient. This is manifest as pseudo orbital proptosis, flat cheek bones and can include an overall midface deficiency. In short this makes the eye stick out further than the underlying bone in profile view, hence the name ‘negative orbital vector’.
In complete correction of a negative orbital vector, the full skeletal deficiency should be ideally addressed. This means it is not a isolated cheek, infraorbital, or orbital floor deficiency but rather a composite of all of these areas. The well known and described ZMC complex (zygomatico-orbtial-maxillary) as a unit os deficient and must be addressed. While standard cheek and infraornitak implants provide a limited effect they are unable to provide a complete skeletal correction.
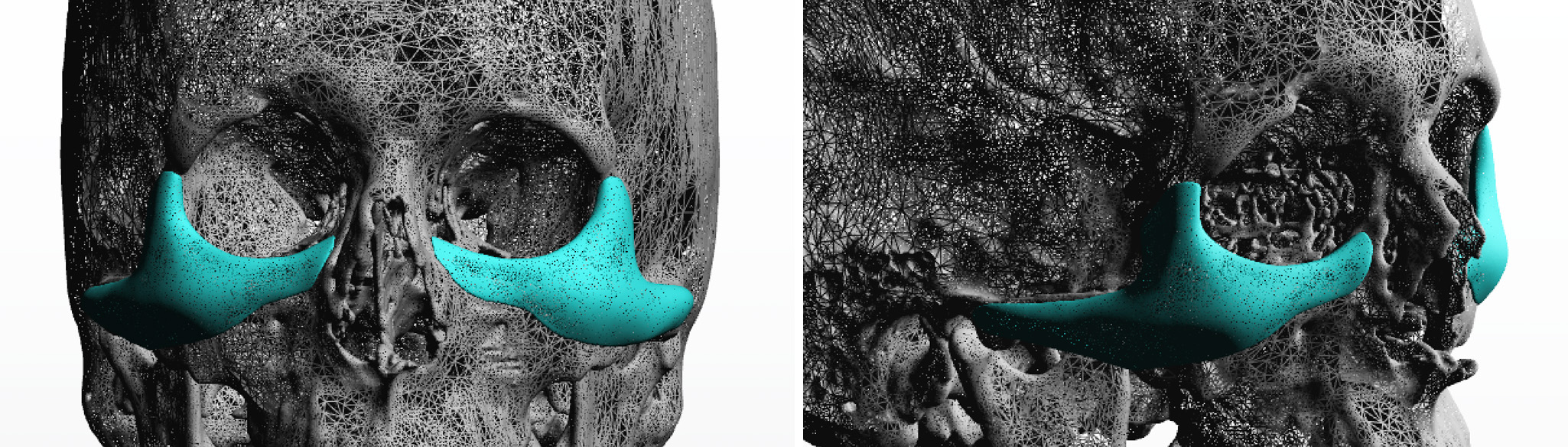
 Case Study: This young male had a recessed lower orbit with a negative orbital vector and flatter cheeks. He desired sting augmentation along the infraorbital rim as well as out onto the cheekbone and extending back along the zygomatic arch.
Case Study: This young male had a recessed lower orbit with a negative orbital vector and flatter cheeks. He desired sting augmentation along the infraorbital rim as well as out onto the cheekbone and extending back along the zygomatic arch.
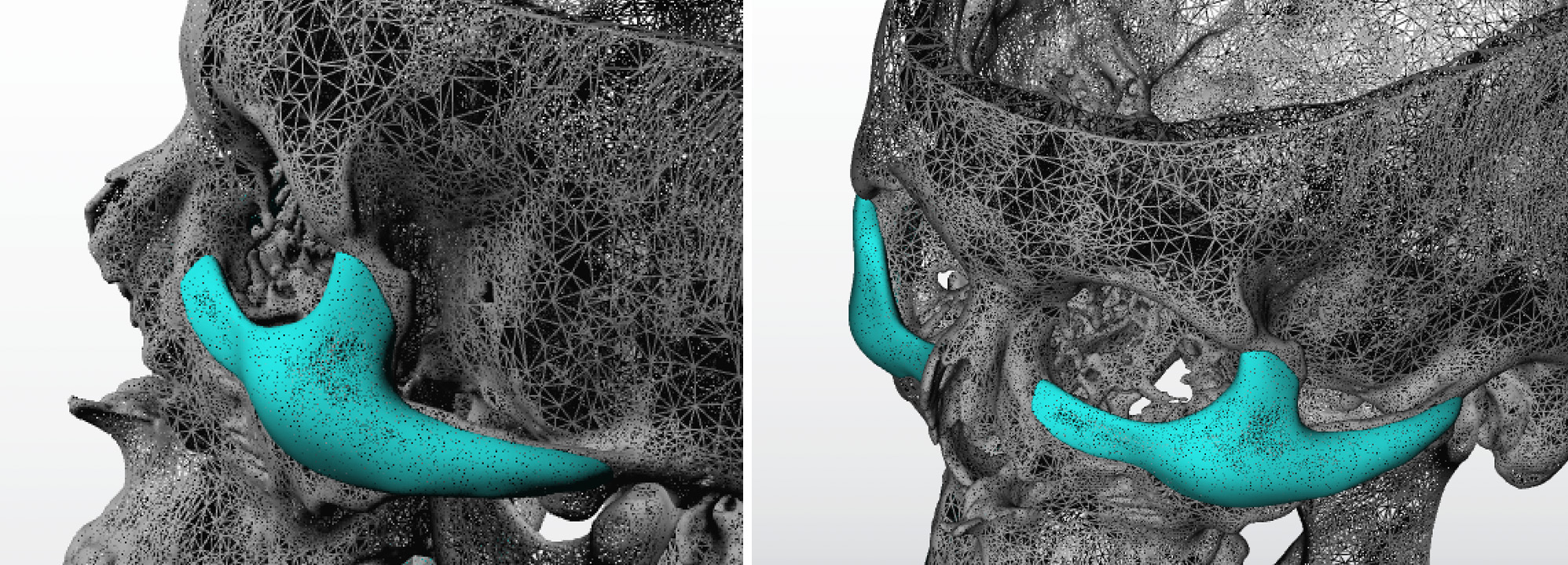
 Because of the degree of inferior orbital and anterior malar augmentation, it was also necessary to extend the implant design up along the lateral orbital rim to ensure that it looked natural and did not create a hollow by the side of the eye.
Because of the degree of inferior orbital and anterior malar augmentation, it was also necessary to extend the implant design up along the lateral orbital rim to ensure that it looked natural and did not create a hollow by the side of the eye.
 Under general anesthesia and through a subciliary incision with a 3mm lateral canthal extension, subperiosteal dissection was done over all required bony areas including back along teh arch to the ear. (posterior temporal process0. The custom implants were inserted, positioned and then secured by two microscrews into the infraorbital rims per side. Orbicularius muscle resuspension and lateral canthopexies were done at the time of lower eyelid closure.
Under general anesthesia and through a subciliary incision with a 3mm lateral canthal extension, subperiosteal dissection was done over all required bony areas including back along teh arch to the ear. (posterior temporal process0. The custom implants were inserted, positioned and then secured by two microscrews into the infraorbital rims per side. Orbicularius muscle resuspension and lateral canthopexies were done at the time of lower eyelid closure.
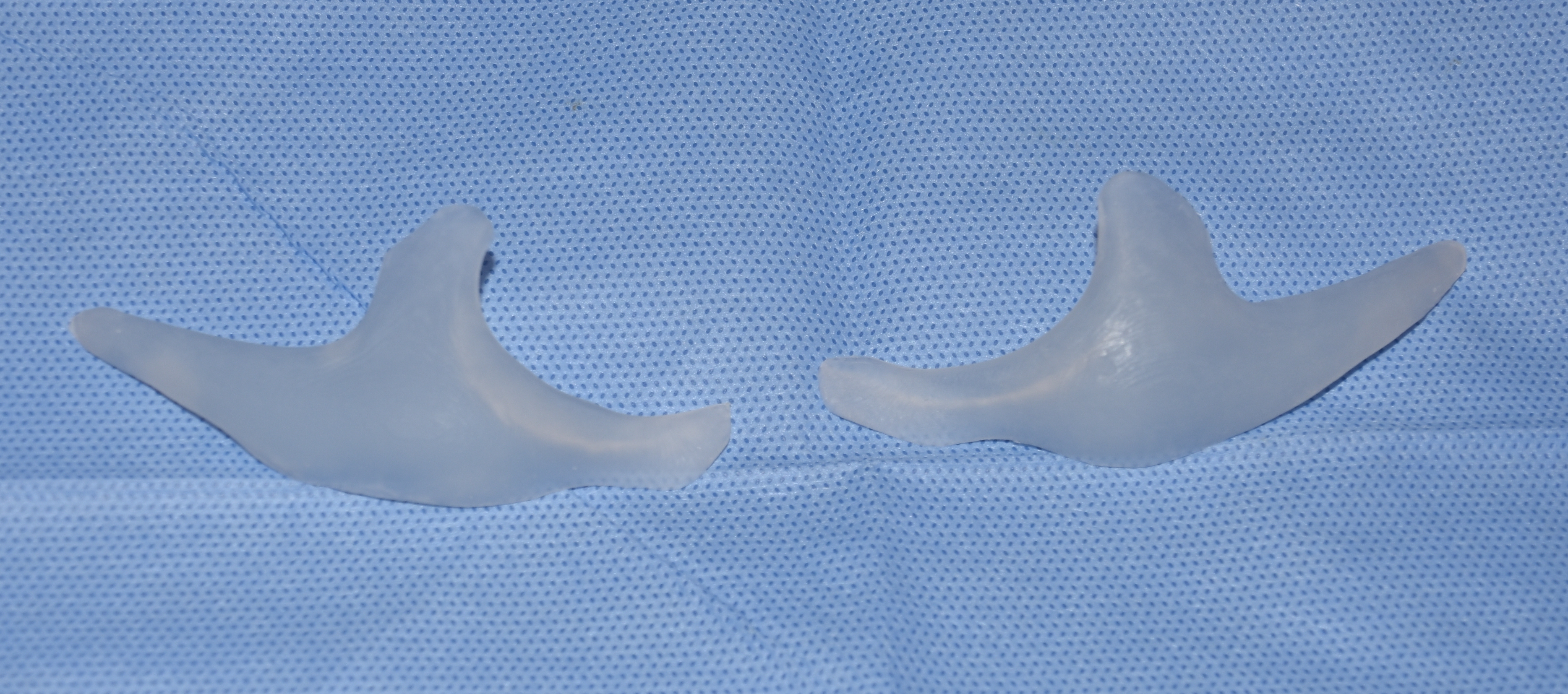
Custom infraorbital-malar implants can effectively recreate a new ZMC complex through an inlay approach. This is a far superior approach using standard implants or some form of orbito-malar osteotomies.
Case Highlights:
1) Custom infraorbital-malar implants typically augment the linear line along the eye back along the zygomatic arch.
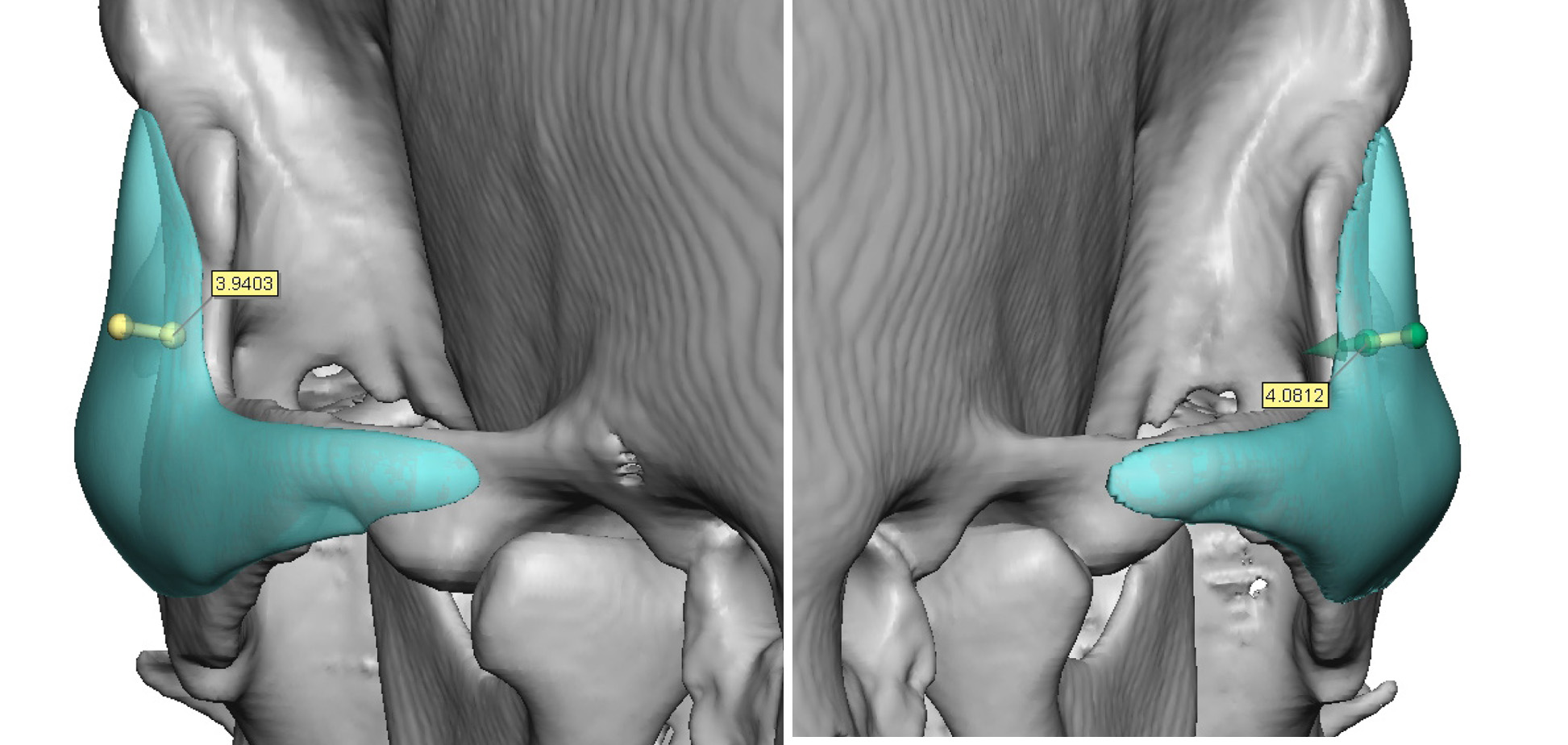
2) How much a custom implant augments along the interior orbital rim is a matter of personal preference and aesthetic needs.
3) Including the lateral orbital rim in a custom infraorbital-malar implant provides a more complete augmentation to the negative orbital vector patient.
Dr. Barry Eppley
Indianapolis, Indiana