

Background: The jaw angle is the intersection of the vertical and horizontal components of the non-tooth bearing part of the lower jaw. Its development and size add a structural feature to the lower face whose prominence is usually viewed as a favorable feature for either men or women. Once developed the jaw angle bone changes little as one ages unlike the tooth bearing part of the lower jaw.
The well known sagittal split mandibular ramus osteotomy (SSRO) is the most commonly performed elective lower jaw osteotomy. Its primary purpose is to move the lower jaw forward or backward to improve the alignment of the dentition. In doing so the ramus (jaw angle bone) is split longitudinally into a proximal (tooth-bearing) and distal (joint containing) bone segments in a sagittal direction. It is an incredibly clever facial bone procedure that is highly effective.
But its execution requires repositioning and fixing together the two lower jaw bone segments in a new alignment. In addition the proximal bone segment (which constitutes the jaw angle) has extensive subperiosteal tissue stripping down on it to perform the procedure and thus undergoes some significant devascularization. Both maneuvers can cause potential shape changes of the jaw angle due to either a positioning change of the bone or loss of some bone due to resorption after surgery.
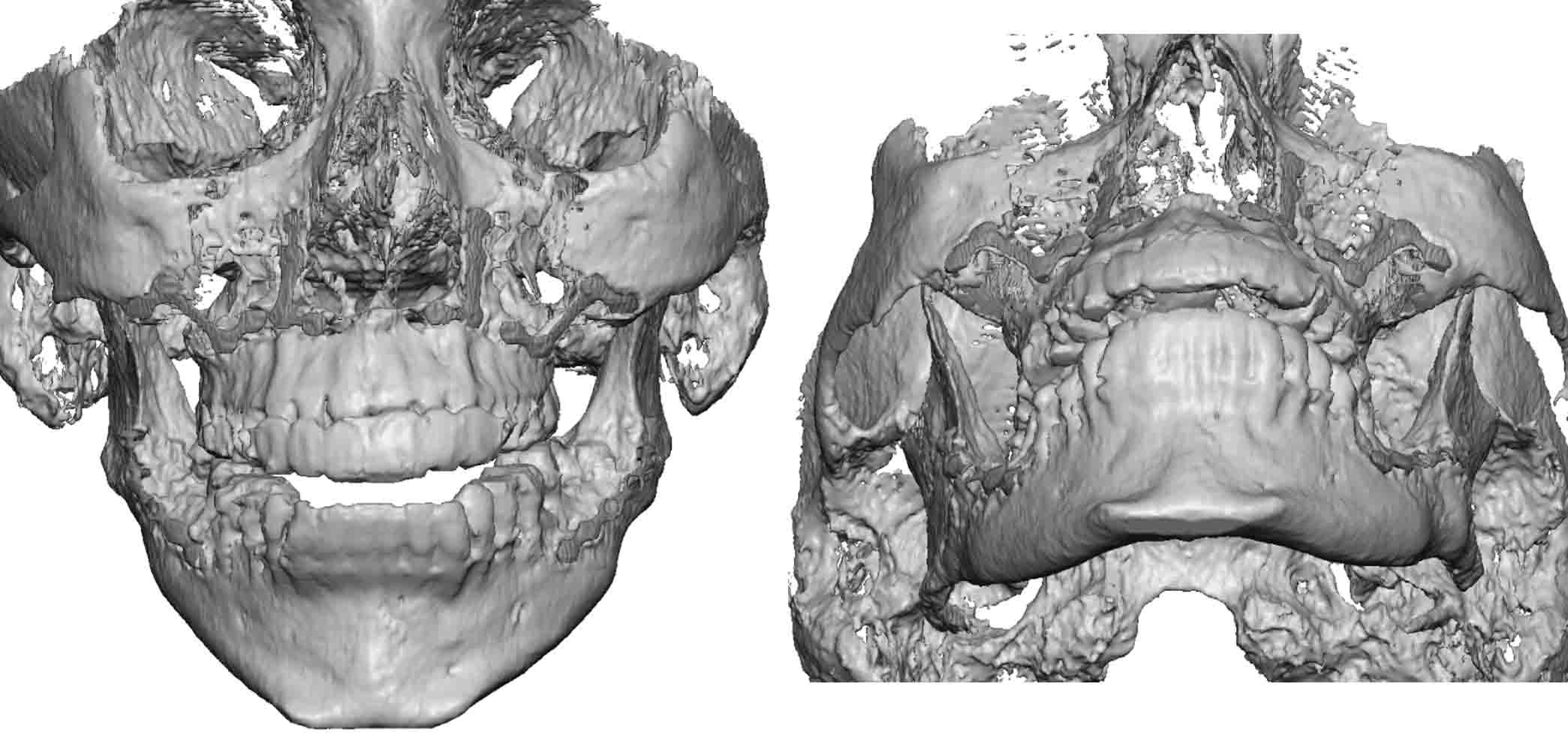
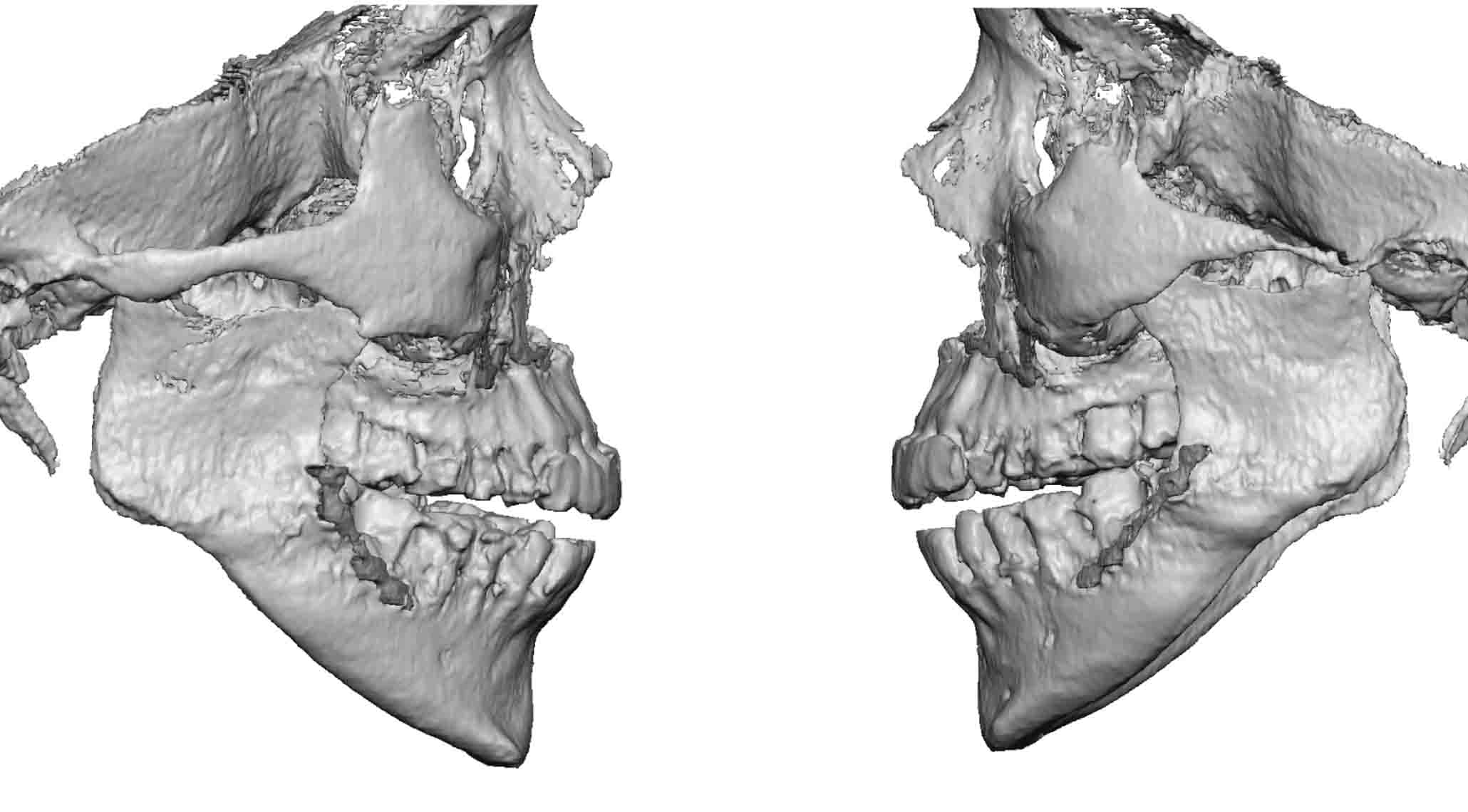 Case Study: This middle aged female had a history of two prior sagittal split mandibular osteotomies years previously. After the surgeries her jaw angle shape changed (was lost) and it had become more evident as she aged and loose tissue developed along the jawline and neck. The loss of jaw angle shape was greater on the left than the right. A 3D CT scan showed the jaw angle malformations.
Case Study: This middle aged female had a history of two prior sagittal split mandibular osteotomies years previously. After the surgeries her jaw angle shape changed (was lost) and it had become more evident as she aged and loose tissue developed along the jawline and neck. The loss of jaw angle shape was greater on the left than the right. A 3D CT scan showed the jaw angle malformations.
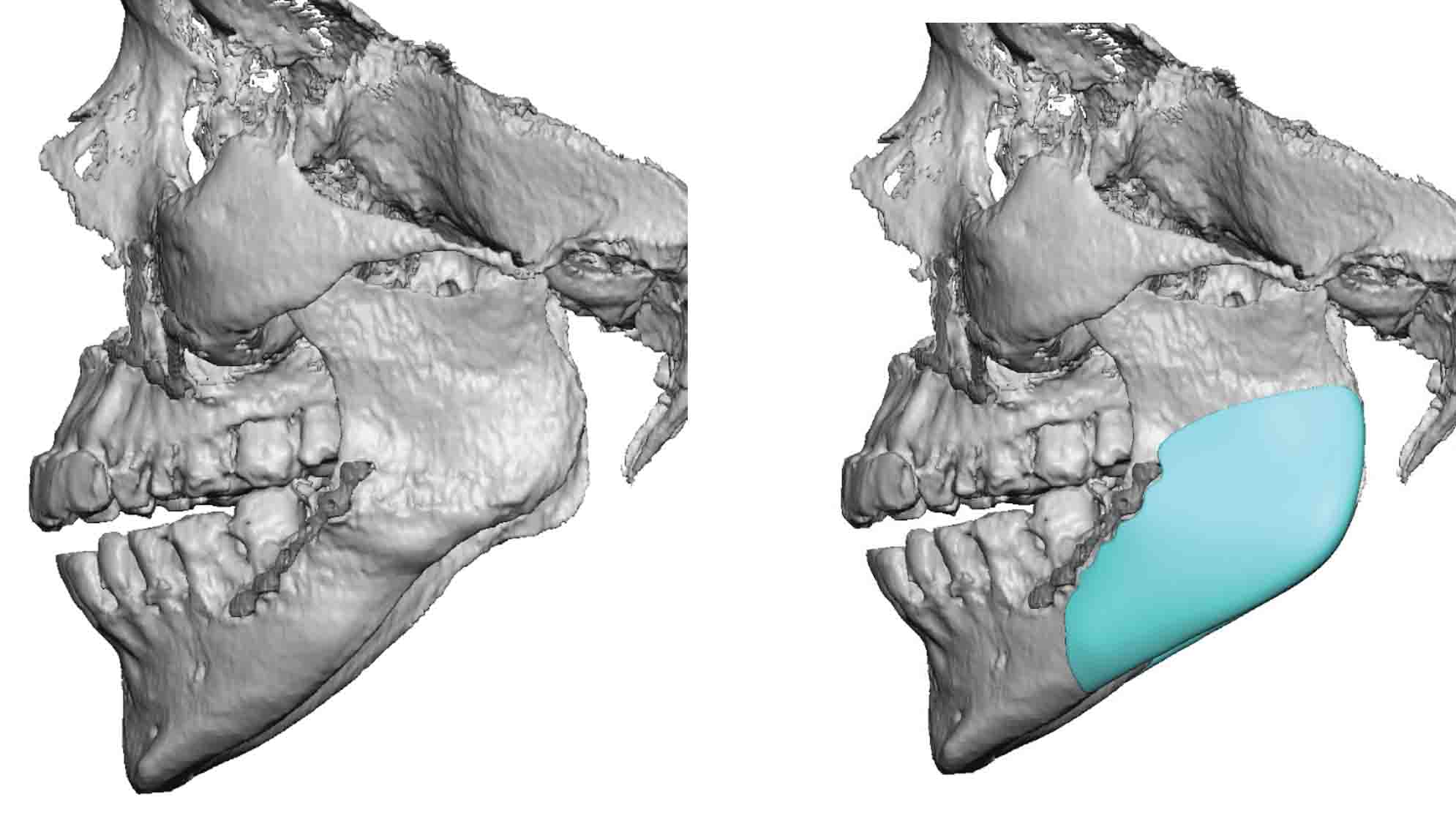
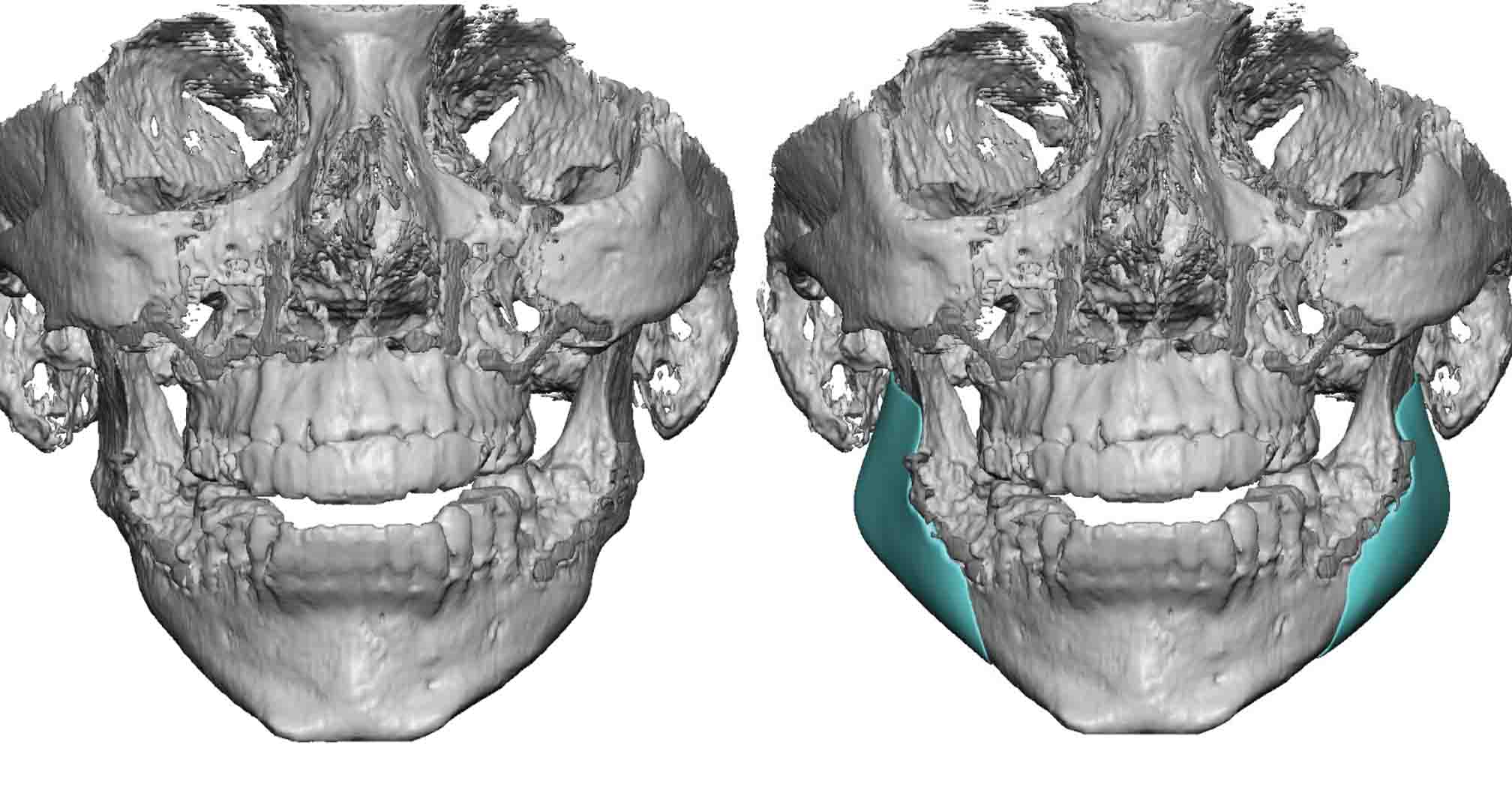
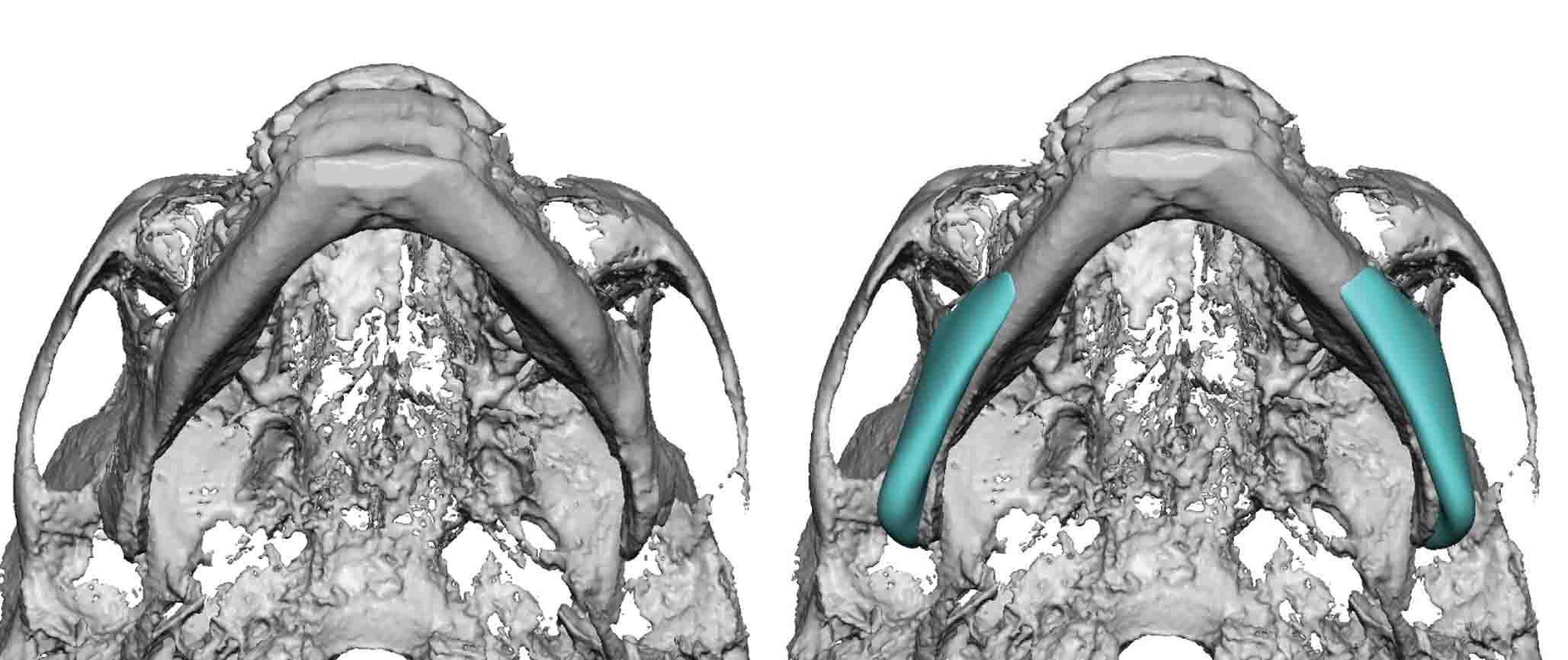
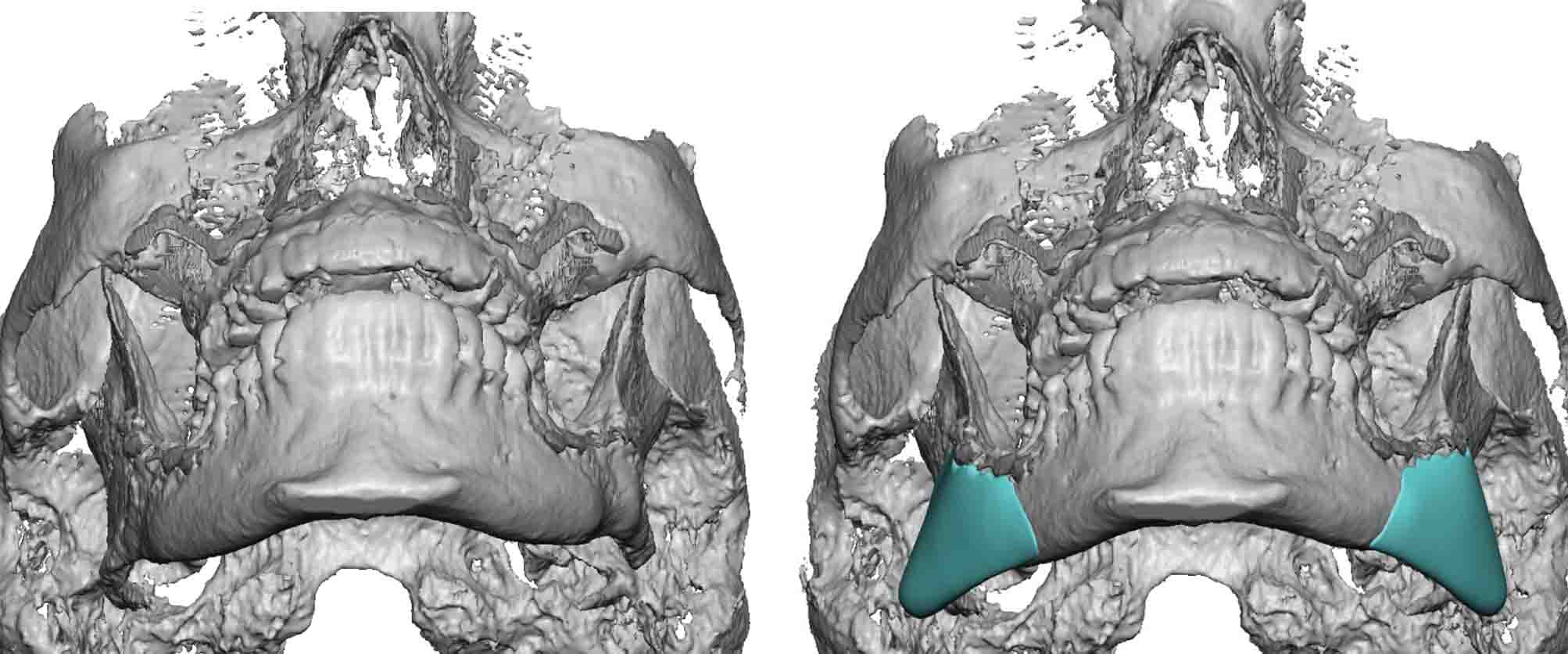 Using the 3D CT scan custom jaw angle implants were designed to not only secondarily reconstruct the jaw angle shape but probably make them more pronounced than they were originally.
Using the 3D CT scan custom jaw angle implants were designed to not only secondarily reconstruct the jaw angle shape but probably make them more pronounced than they were originally.

 Under general anesthesia, markings on her face shows the outline of her existing jaw angles and their new location with the placement of the custom jaw angle implants. Her original posterior vestibular intraoral incisions were re-opened and the jaw angle exposed. Metal fixation plates and screws were evident and these plates, as per the implant design, were used to position the implants into their desired position and help stabilize them for two point screws fixation.
Under general anesthesia, markings on her face shows the outline of her existing jaw angles and their new location with the placement of the custom jaw angle implants. Her original posterior vestibular intraoral incisions were re-opened and the jaw angle exposed. Metal fixation plates and screws were evident and these plates, as per the implant design, were used to position the implants into their desired position and help stabilize them for two point screws fixation.
Highlights:
1) Sagittal split mandibular osteotomies have the potential to alter the shape of the jaw angle due to either segmental repositioning or some any resorption.
2) Secondary reconstruction of the atrophic jaw angle is best done by custom jaw angle implants.
3) The indwelling fixation hardware from the sagittal split mandibular osteotomy serves as a registration for custom jaw angle implant placement.
Dr. Barry Eppley
Indianapolis, Indiana