

Background: There are variety of conditions that can cause bony deformities of the angle region of the lower jaw. Abnormal growth from congenital/developmental causes, traumatic injuries and elective jaw surgery can all adversely affect the shape of the jaw angles. By far in my experience elective osteotomies in orthognathic surgery cause the greatest array of bine shape changes by the sheer number of such procedures that are performed.
The osteotomy types for moving the jaw forward or back are either the commonly used sagittalsplit ramus osteotomy (SSRO) and the older vertical oblique osteotomy (VO) which is used for setbacks only. Both involve cutting through he ramus and then putting the bone segments back together albeit with some differences in the shape of the ramus with the forward or backward movement of the distal tooth-bearing bony segment.
While bony healing almost always occurs in ramus osteotomies that does not mean their preoperative shape remains unchanged. While the ultimate success of orthognathic surgery is defined by the establishment of a normal and stable occlusion, the shape of the lower jaw does change in both favorable and unfavorable ways. While the chin in the front of the jaw is often improved by increased projection, the jaw angles in the back may lose some other angular or prominent appearance.
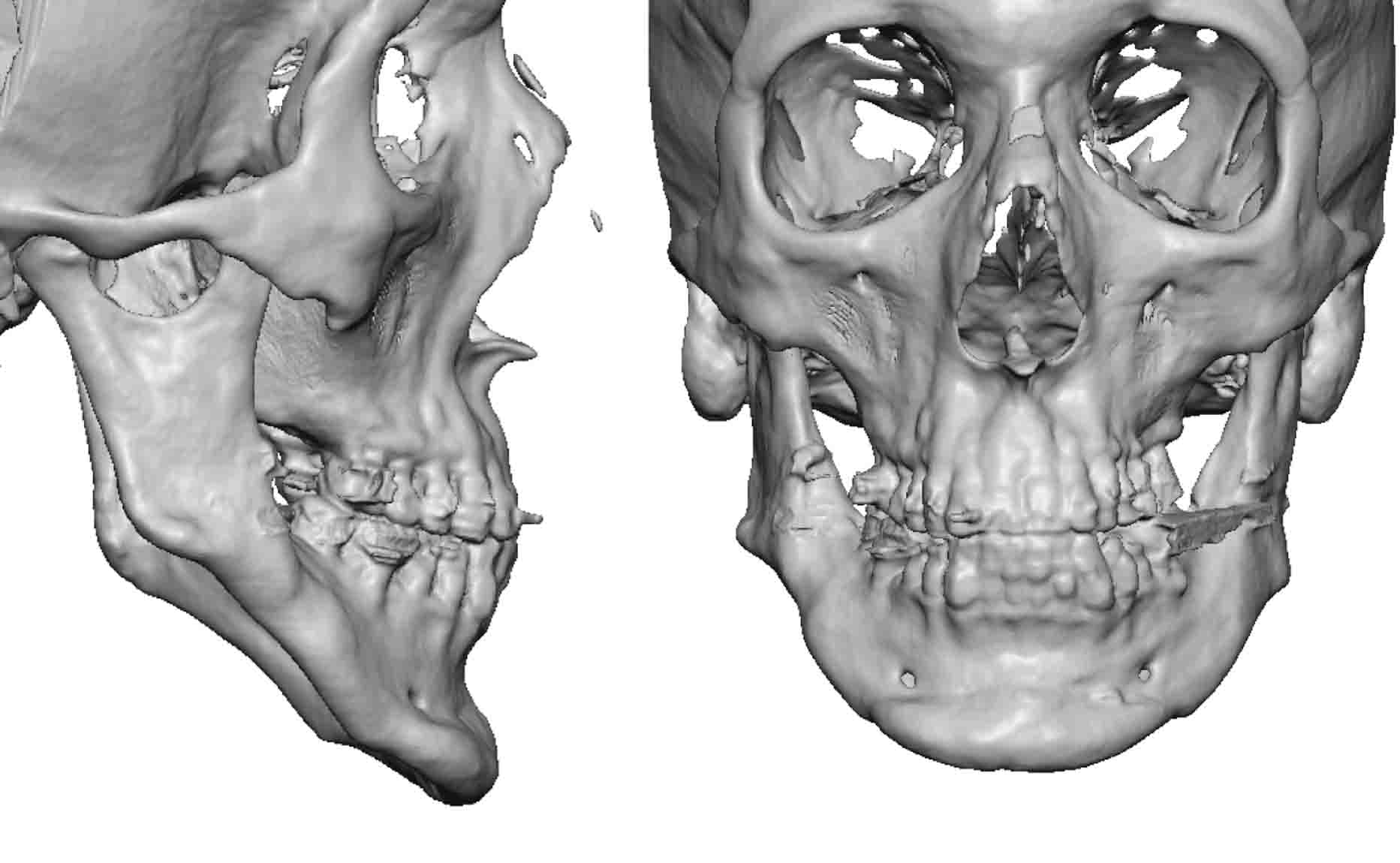 Case Study: This older male has long been bothered by the shape of his lower jaw. He had a ‘short’ lower jaw which was manifest as jaw angles that looked completely missing. He has undergone lower jaw orthognathic surgery as a younger man although it was unclear as to what type of osteotomy it was. His 3D CT scan showed very high jaw angles with a mandibular plane angle that was in the range of 60 degrees with an obvious asymmetry between the back and front the jaw as evidenced by the irregular inferior border line.
Case Study: This older male has long been bothered by the shape of his lower jaw. He had a ‘short’ lower jaw which was manifest as jaw angles that looked completely missing. He has undergone lower jaw orthognathic surgery as a younger man although it was unclear as to what type of osteotomy it was. His 3D CT scan showed very high jaw angles with a mandibular plane angle that was in the range of 60 degrees with an obvious asymmetry between the back and front the jaw as evidenced by the irregular inferior border line.
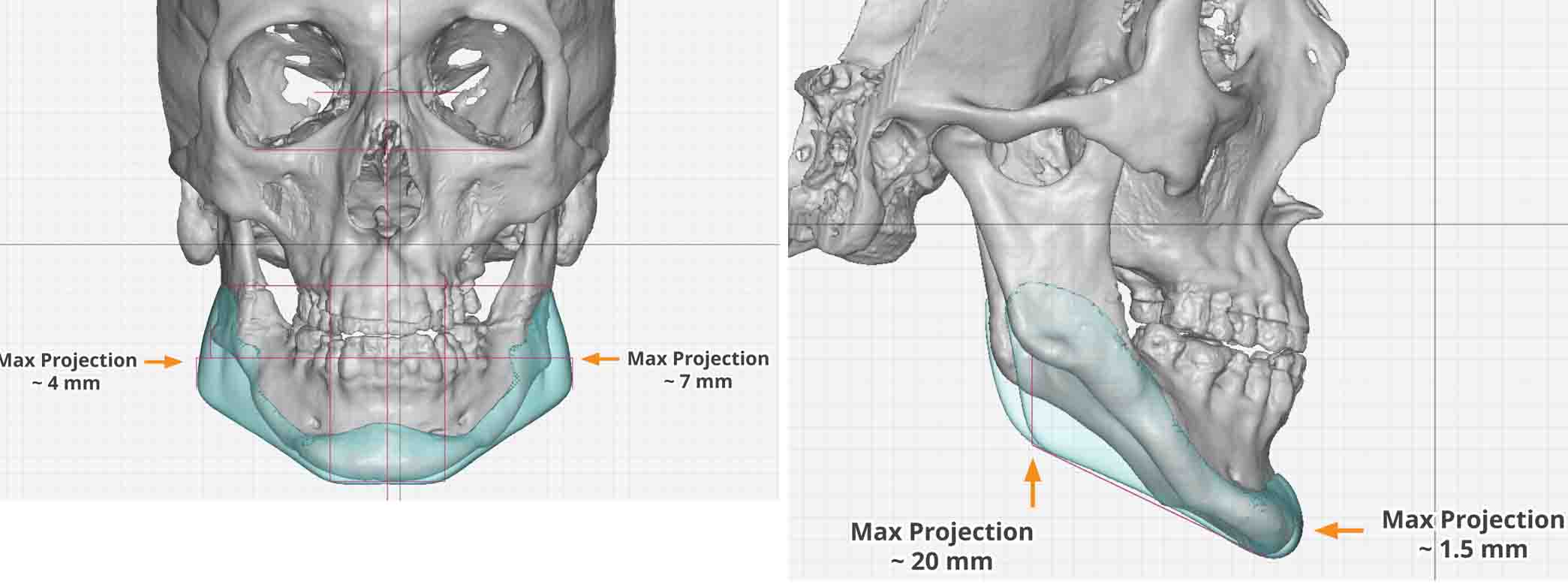 A custom jawline implant was made that vertically lengthened his jaw angle by 20mms with minimal added horizontal chin projection.
A custom jawline implant was made that vertically lengthened his jaw angle by 20mms with minimal added horizontal chin projection.
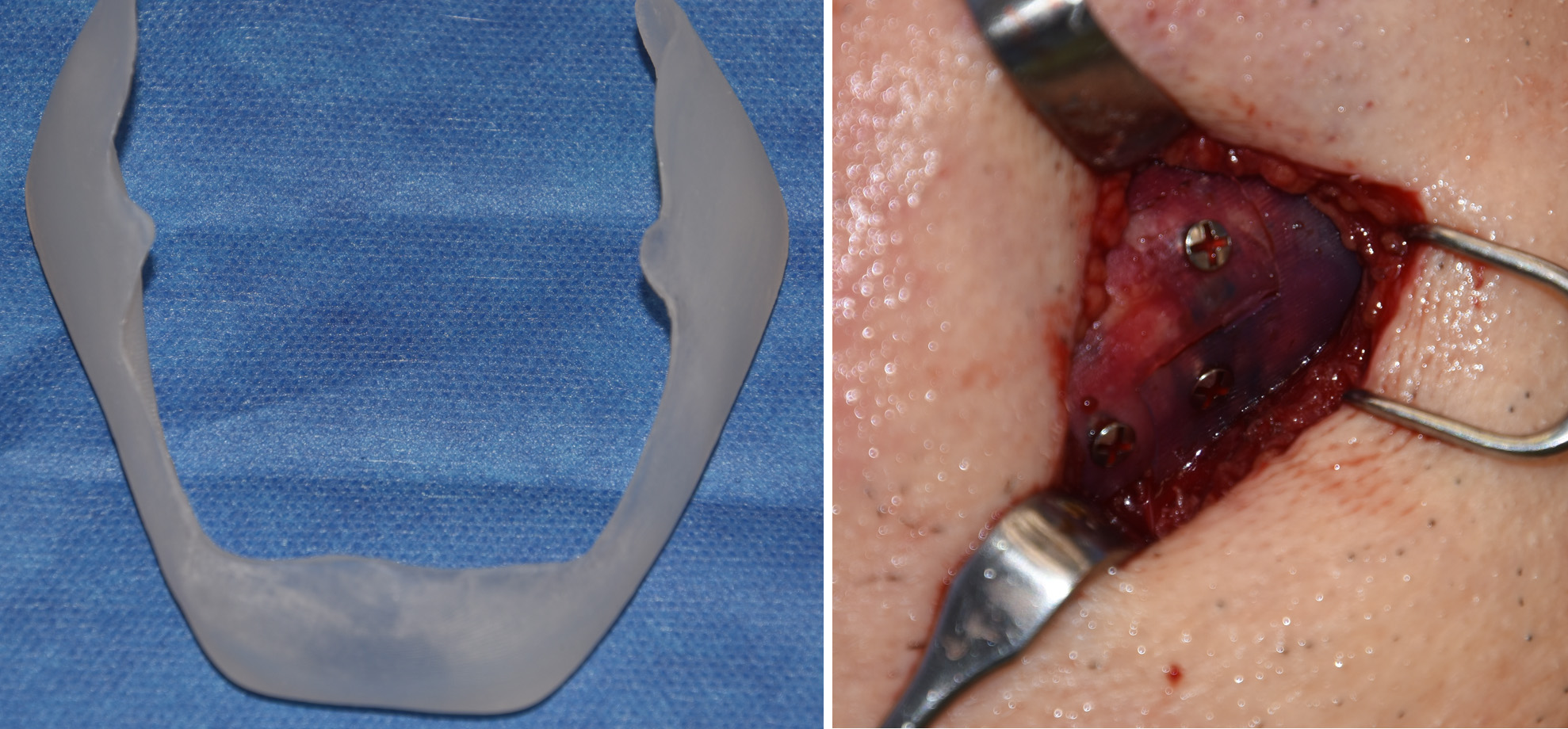 Under general anesthesia and through a combined submental skin and intraoral posterior vestibular incisions, the custom jawline implant as placed in a split fashion in a back to front placement method due to the size of the jaw angles. The implant was reunited in the midline within geometric split technique with screw fixation.
Under general anesthesia and through a combined submental skin and intraoral posterior vestibular incisions, the custom jawline implant as placed in a split fashion in a back to front placement method due to the size of the jaw angles. The implant was reunited in the midline within geometric split technique with screw fixation.

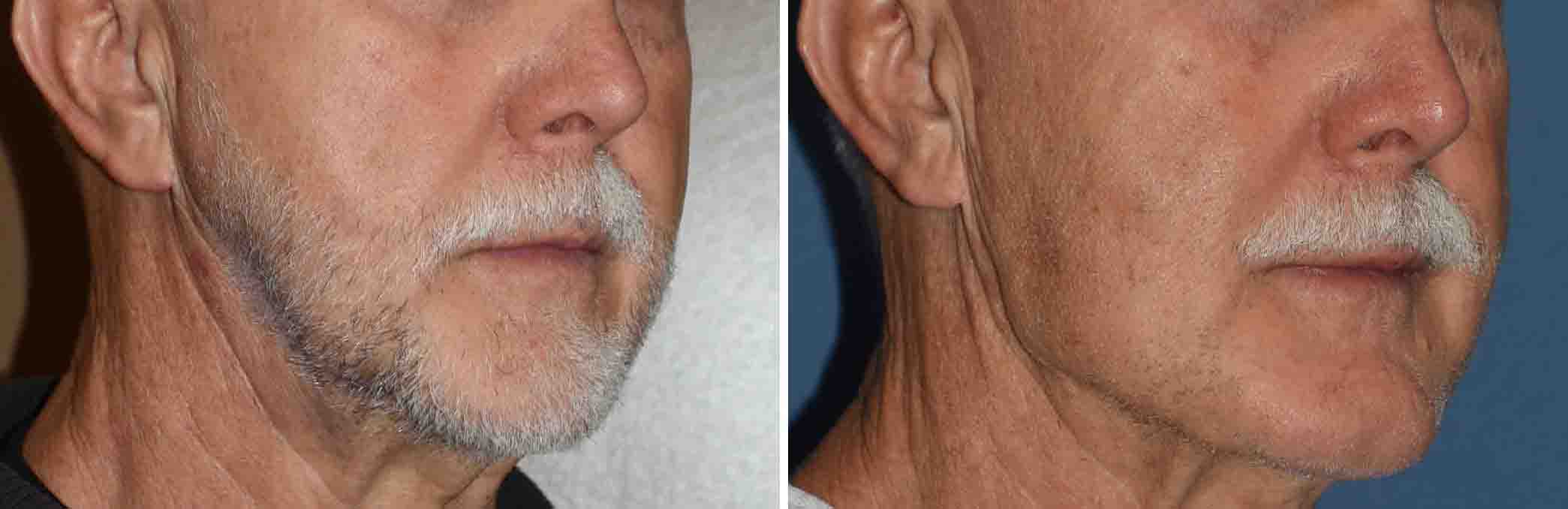
 His intraoperative result showed a substantial lengthening of the jaw angles that connected in a more linear fashion with the anterior chin. There was no evidence of any masseteric muscle dehiscence.
His intraoperative result showed a substantial lengthening of the jaw angles that connected in a more linear fashion with the anterior chin. There was no evidence of any masseteric muscle dehiscence.
Case Highlights:
1) Older men can have a custom jawline implant just as successfully as much younger men.
2) Significant vertical jaw angle lengthening can be done with a custom jawline implant with a low risk of masseteric muscle dehiscence with careful surgical technique.
3) Deformed jaw angles can be reconstructed with a custom implant design.
Dr. Barry Eppley
Indianapolis, Indiana