

Background: The mandibular plane angle is a term frequently used in dentistry particularly in orthodontics and cephalometric analysis. Technically it is called the Frankfort mandibular plane angle and is formed by the intersection of the Frankfort horizontal plane and the mandibular plane. These intersecting lines create an angle of which a measurement of 25 +/- 5 degrees would be considered normal. A high plane angle would be 30 degrees or more and a low plane angle patient would be 20 degrees or less. The relevance of this in orthodontics is that a high plane angle is associated with open bites and a low plane angle with closed bites.
But looking beyond the intraoral occlusal ramifications, the mandibular plane angle has external aesthetic facia effects as well. A high plane angle patient can look like they are missing the back part of the jaw with a posterior lower facial deficiency. Conversely the low mandibular plane angle patient usually has a full or prominent jaw angle appearance although the lower face may appear vertically short.
It is the high jaw angle patient that often presents for jawline augmentation. They feel that the jaw angle point is too close to the earlobe or that part of the jaw is absent and gives their face a too narrow appearance. Such a high jaw angle appearance can also result from jaw advancement surgery where the ramus is split into two pieces and re-assembled after the teeth are put into proper occlusion. Such manipulations of the jaw angle bone can result in deformations or loss of part of the jaw angle bone structure.
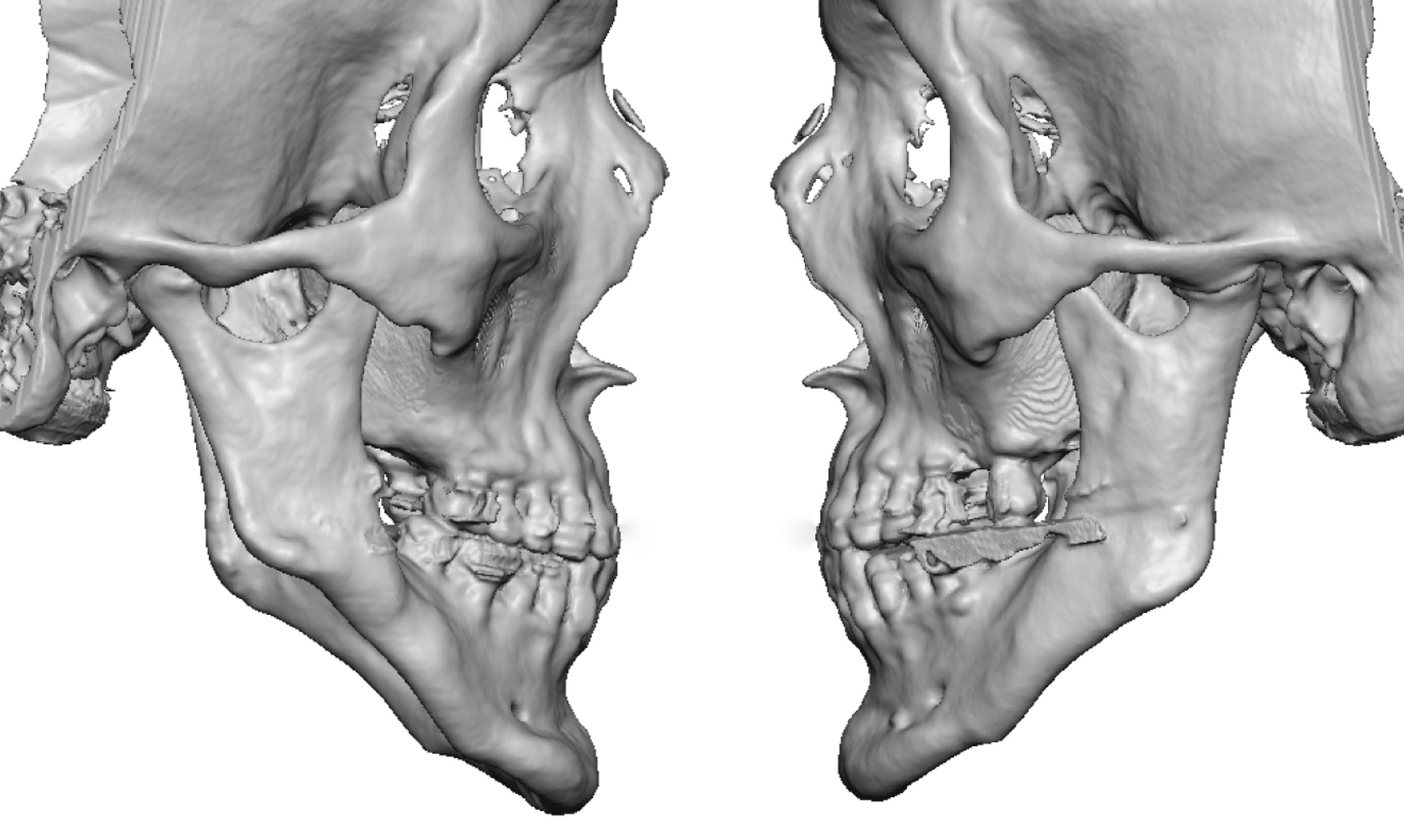 Case Study: This older male was bothered by his very high jaw angles and thin narrow face. He was largely content with his chin position both horizontally and vertically. He had a past history over twenty years ago of undergoing a mandibular advancement surgery for a ‘short jaw’. His 3D CT scan showed how high his jaw angles were with a mandibular plane angle that approximated 45 degrees.
Case Study: This older male was bothered by his very high jaw angles and thin narrow face. He was largely content with his chin position both horizontally and vertically. He had a past history over twenty years ago of undergoing a mandibular advancement surgery for a ‘short jaw’. His 3D CT scan showed how high his jaw angles were with a mandibular plane angle that approximated 45 degrees.
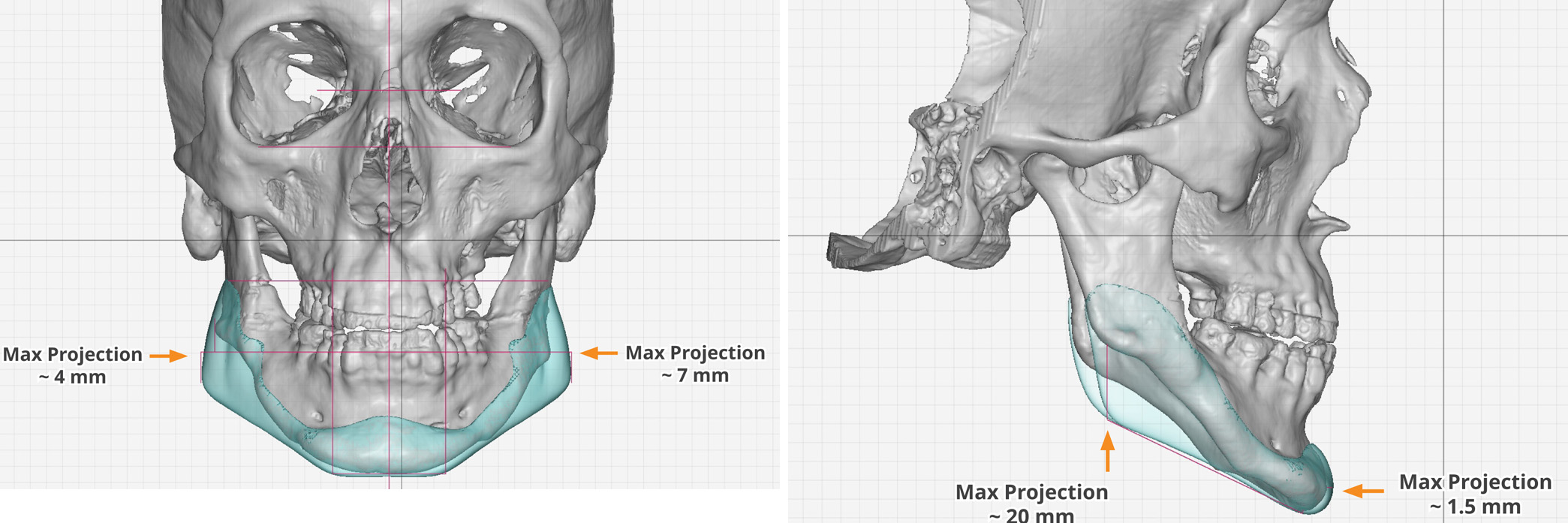
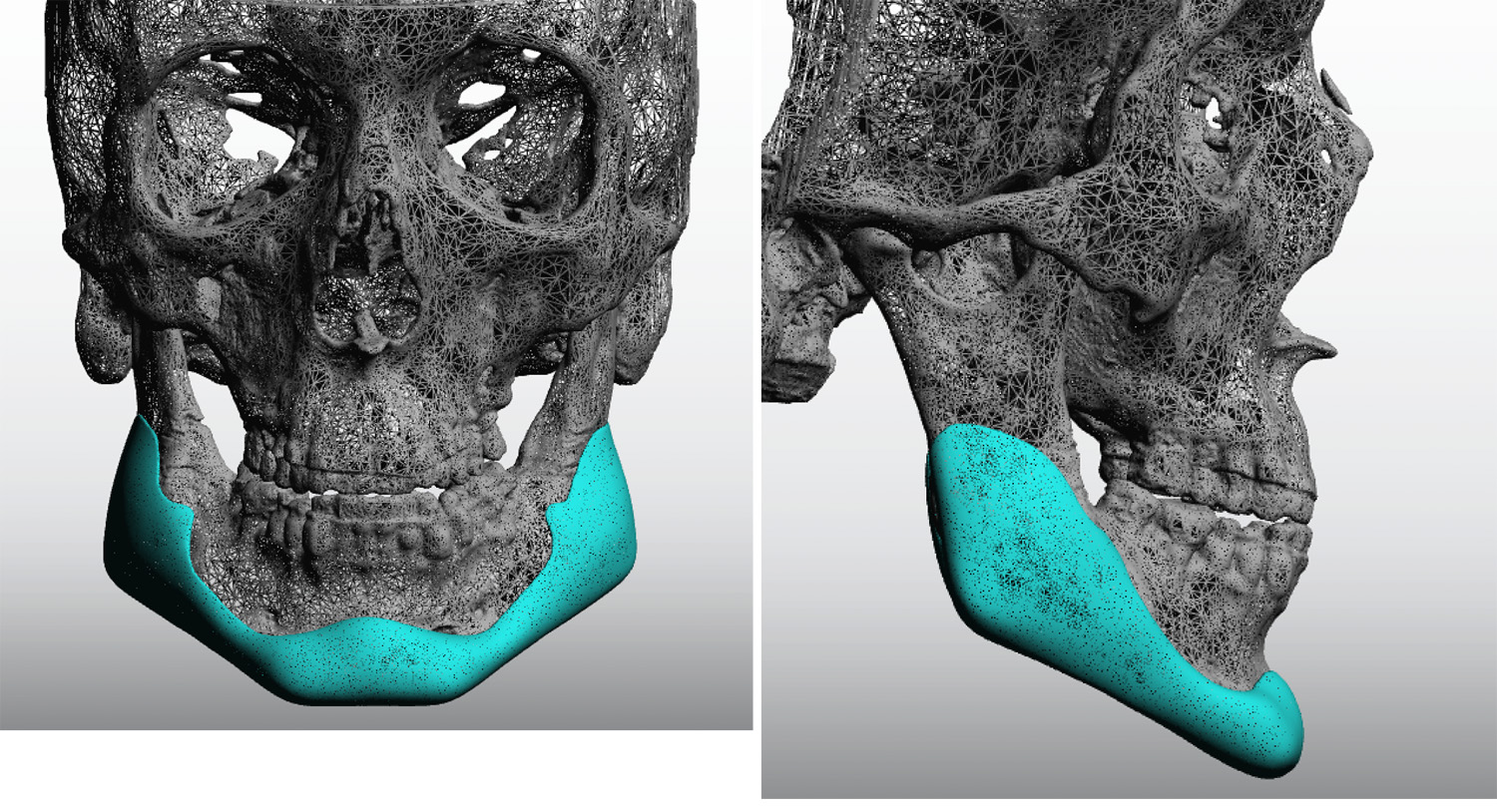 Using his 3D CT scan a custom jawline implant was desired that subsetially dropped down is jaw angles by 20 degrees. He wanted to drop them 30 degrees but I refused with enough concerns about the risk of masseteric muscle disinsertion. His chin changes were very minimal and were mainly there to connect the two sides of the implant.
Using his 3D CT scan a custom jawline implant was desired that subsetially dropped down is jaw angles by 20 degrees. He wanted to drop them 30 degrees but I refused with enough concerns about the risk of masseteric muscle disinsertion. His chin changes were very minimal and were mainly there to connect the two sides of the implant.
 Under general anesthesia a combined submental skin incision and two posterior intraoral incisions were used for placement. Because of the size of the jaw angle portions of the implant the custom jawline implant needed to be split in the midline and placed in a ‘back to front’ technique.
Under general anesthesia a combined submental skin incision and two posterior intraoral incisions were used for placement. Because of the size of the jaw angle portions of the implant the custom jawline implant needed to be split in the midline and placed in a ‘back to front’ technique.
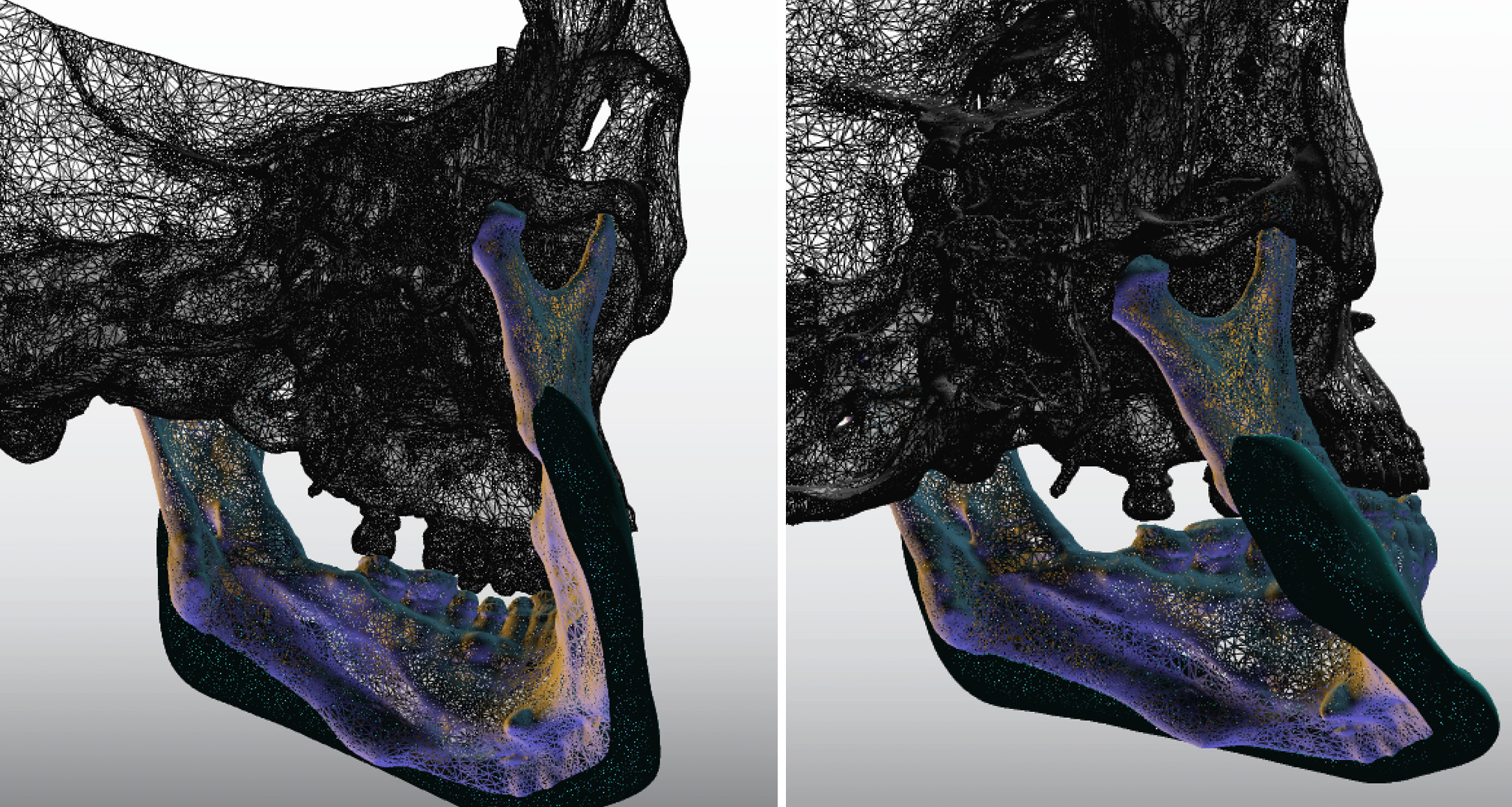 High mandibular plane angle patients require custom jawline implants that vertically lengthen the jaw angles. When the vertical jaw angle lengthening is substantial the risk of the masseter muscle not following downward with the implant is significant. This risk is magnified when the patient has had prior mandibular ramus surgery. But that risk is often necessary to take if one wants to make an appreciable change in the shape of the jawline.
High mandibular plane angle patients require custom jawline implants that vertically lengthen the jaw angles. When the vertical jaw angle lengthening is substantial the risk of the masseter muscle not following downward with the implant is significant. This risk is magnified when the patient has had prior mandibular ramus surgery. But that risk is often necessary to take if one wants to make an appreciable change in the shape of the jawline.
Highlights:
1) High jaw angles may exist naturally or occur after a sagittal split mandibular osteotomy.
2) Substantially dropping down the jaw angles requires a custom jawline implant approach.
3) The risk of massteric muscle disinsertion is much higher when substantial vertical jaw angle lengthening is done particularly after prior mandibular ramus surgery.
Dr. Barry Eppley
Indianapolis, Indiana