

Background: While people have varying amounts of fat in their face, loss of a significant amount of it creates an unnatural and unhealthy look. Known medically as facial lipoatrophy, there are a variety of well known causes from genetics, extreme weight loss, medications side effects effects and certain diseases. Its variable presentations has created a scale assessment of facial lipoatrophy from I to V, with V being the most severe having an extremely gaunt and emaciated looking face.
The treatment options for facial lipoatrophy include varying methods of soft tissue augmentation. The usual options include injectable fillers and fat injections. Longer lasting injectable fillers like Radiesse and Sculptra are preferred as they offer a better result and value in terms of both volume addition and duration. The use of Sculptra is most common in facial lipoatrophy as its development and historic use was for HIV medication induced type IV and V facial lipoatrophy patients with severe wasting.
Fat injections seem the most logical to replace the facial fat that has been lost in facial lpoatrophy. But adequate donor sites may not be available as these patients are often thin with little fat stores. But even with adequate donor fat, transfer to the face is associated with unpredictable and low survival rates. This is no surprise given that it is being injected into facial areas that did retain its natural fat anyway.
Case Study: This middle-aged male had a significant type IV/V facial lipoatrophy. He had previously been through full face fat injections which he started lasted about three weeks with no long term retention. His desire was to improve his mdifacial appearance particularly in the cheek and anterior maxillary areas. As an alternative approach he opted for a permanent implant approach.
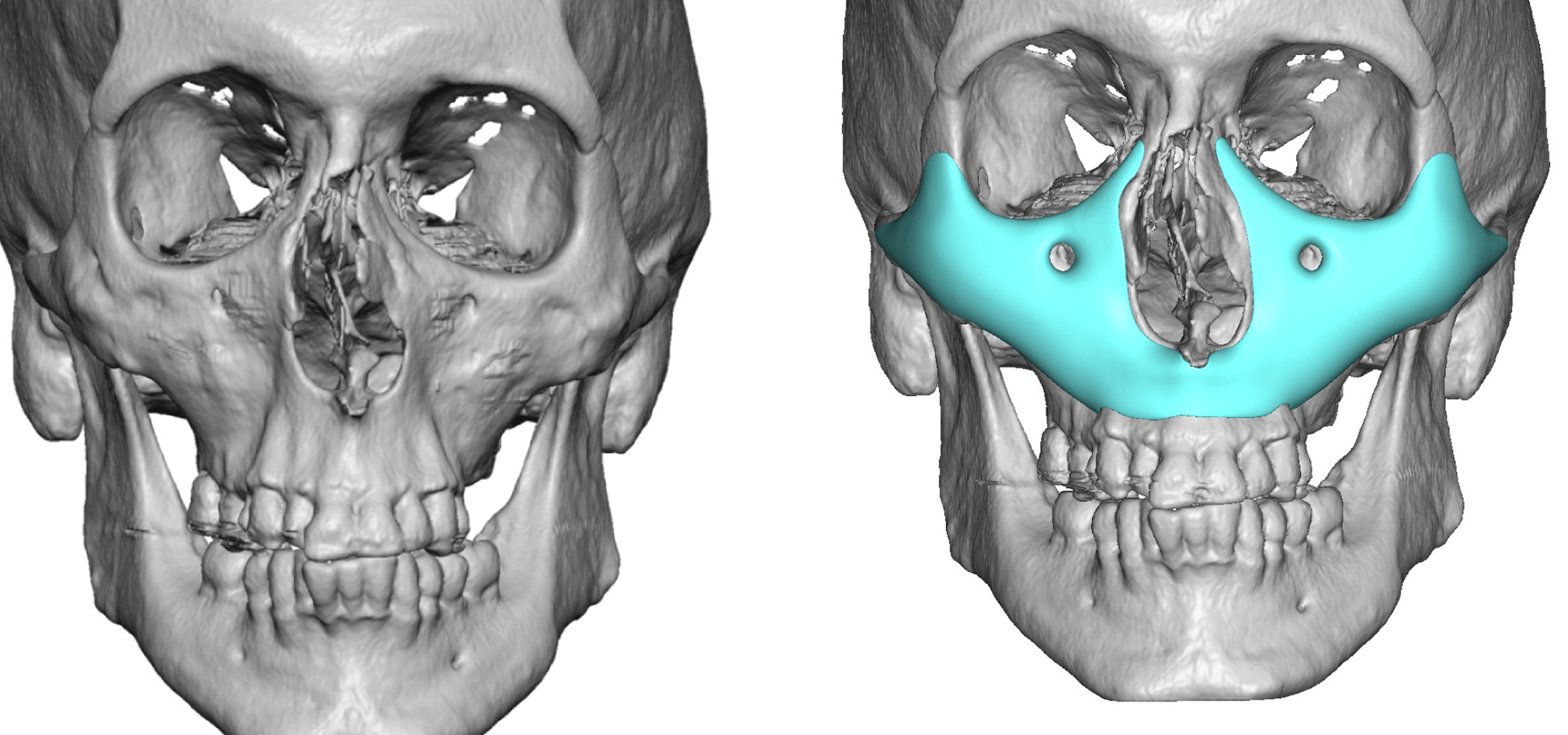
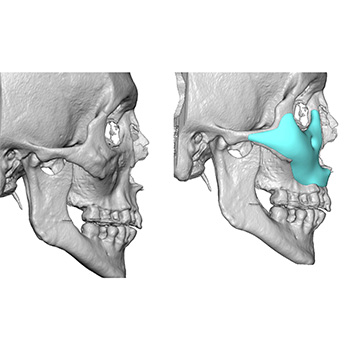
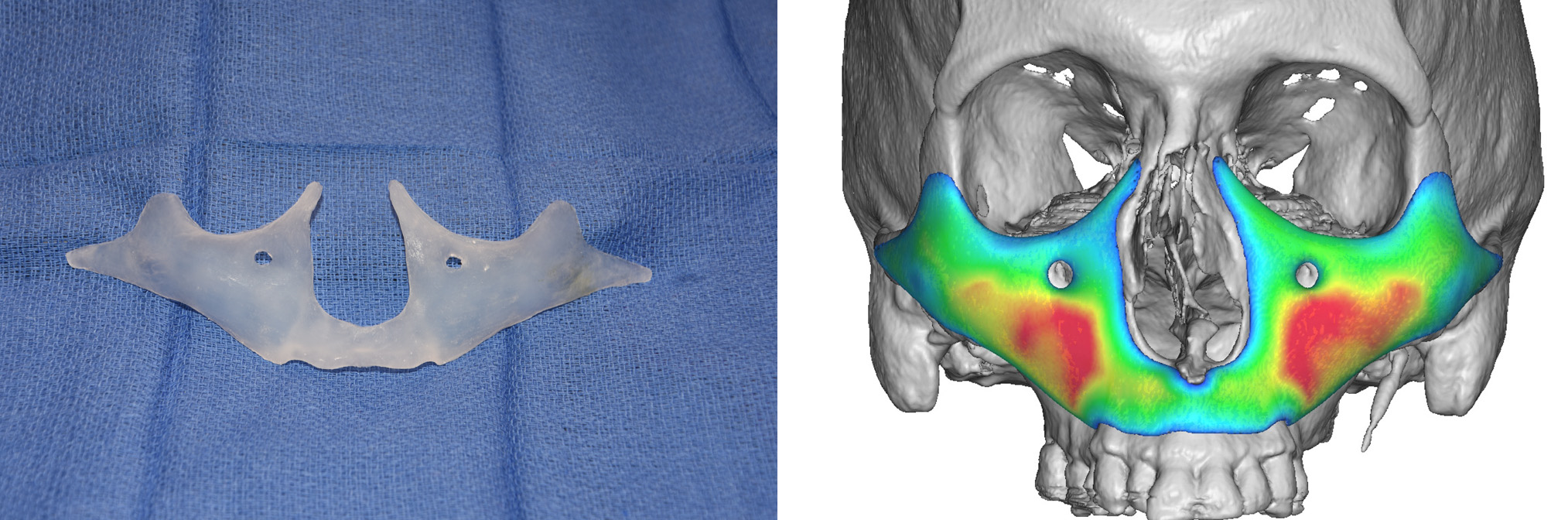
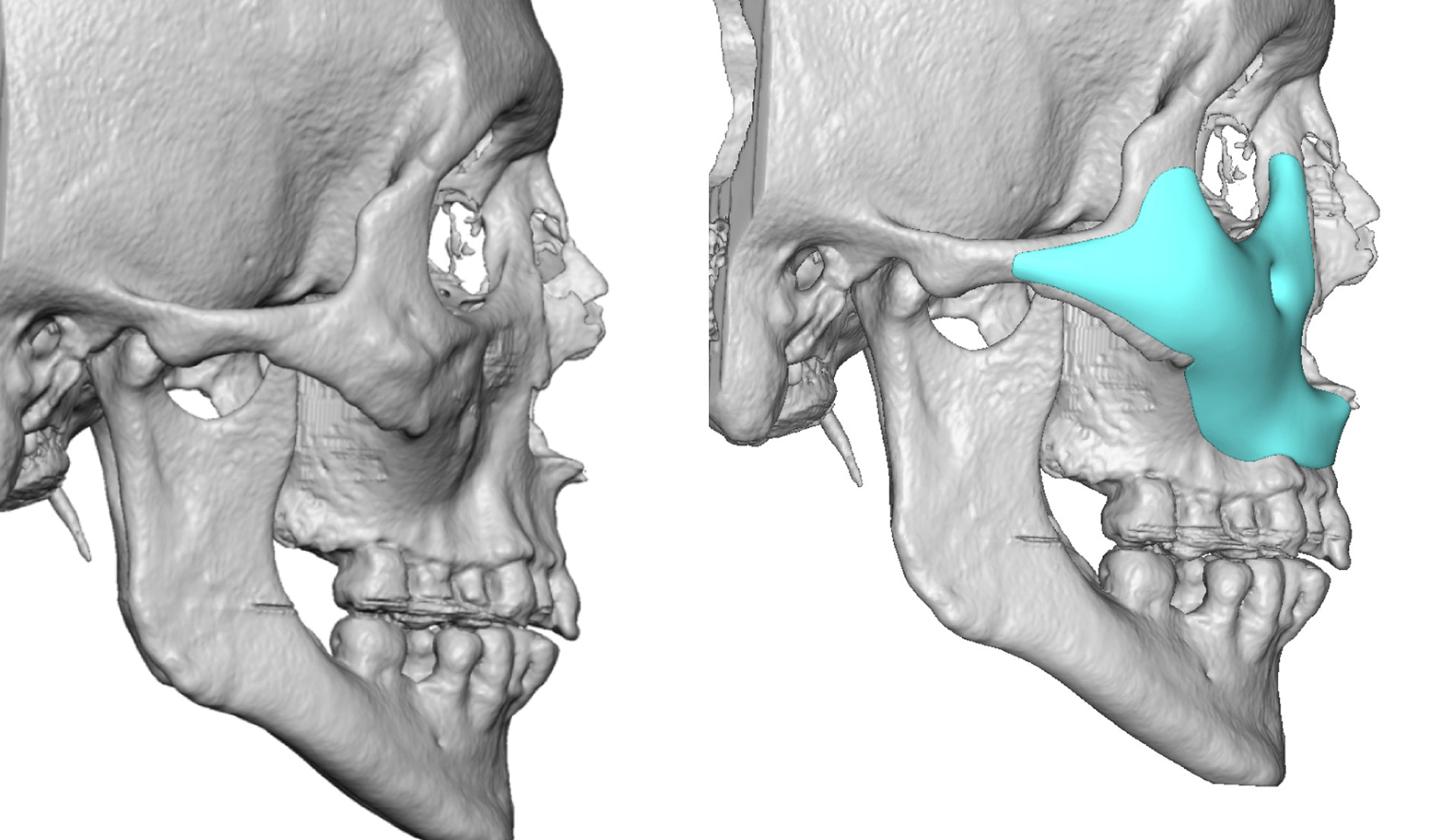 Using the 3D CT scan a custom midface implant was designed to cover all bony surfaces of the midface. It covered the infraorbital over to the nasals bones, done over the maxilla and around the nose as well as across the cheeks out onto the zygomatic arches. Its thickness varied from 6mms in the cheeks to 2mm across the infraorbital rims.
Using the 3D CT scan a custom midface implant was designed to cover all bony surfaces of the midface. It covered the infraorbital over to the nasals bones, done over the maxilla and around the nose as well as across the cheeks out onto the zygomatic arches. Its thickness varied from 6mms in the cheeks to 2mm across the infraorbital rims.
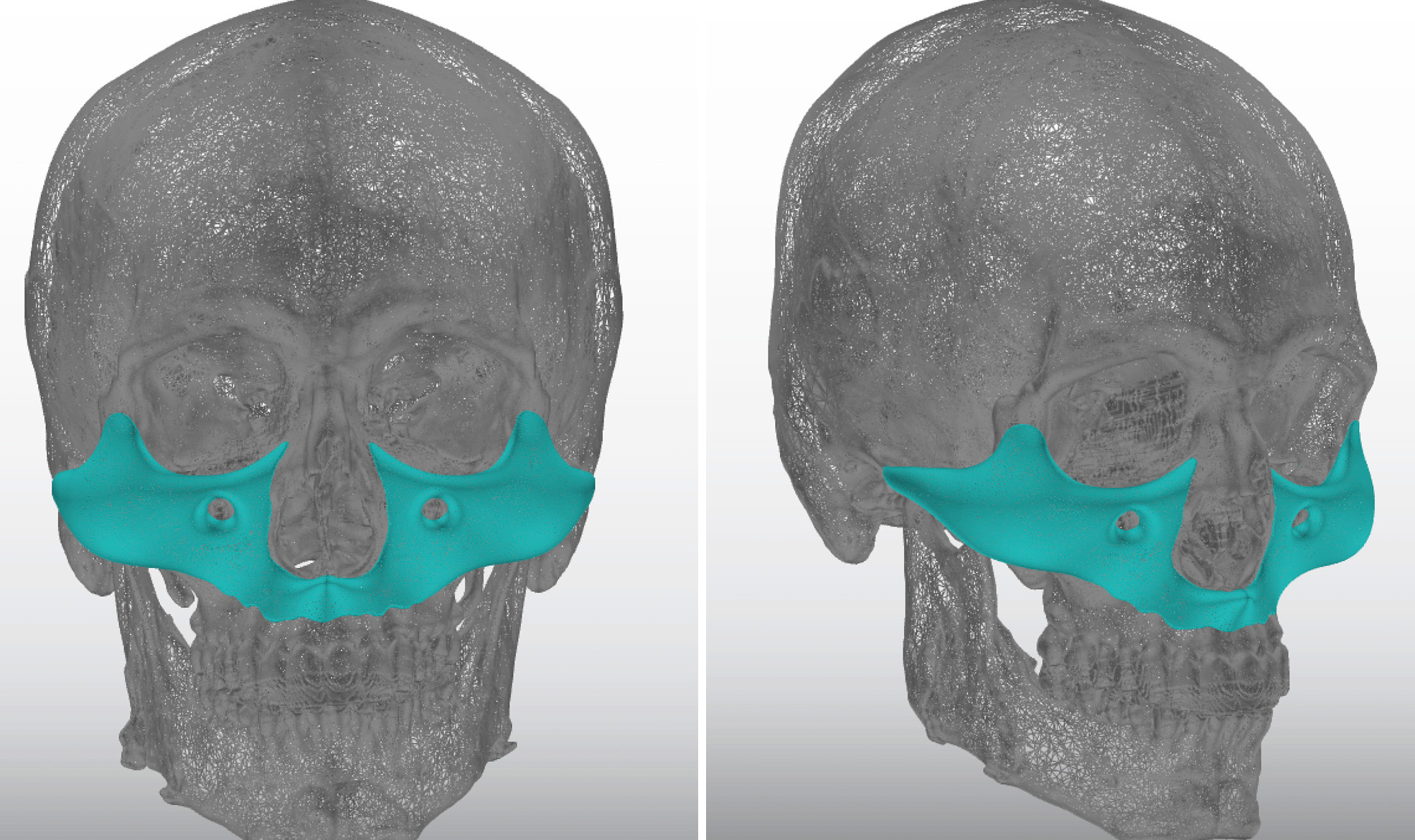 Because of its total coverage of the midface, it looked like a mask. Hence it can be called a custom middle mask implant.
Because of its total coverage of the midface, it looked like a mask. Hence it can be called a custom middle mask implant.
 Under general anesthesia and through combined intraoral and lower eyelid inciseonal approaches, the custom midface implant was placed. It was secured by 1.6mm titanium screws along the infraorbital rim through the eyelid incisions as well as into the maxilla through the intraoral incisions.
Under general anesthesia and through combined intraoral and lower eyelid inciseonal approaches, the custom midface implant was placed. It was secured by 1.6mm titanium screws along the infraorbital rim through the eyelid incisions as well as into the maxilla through the intraoral incisions.
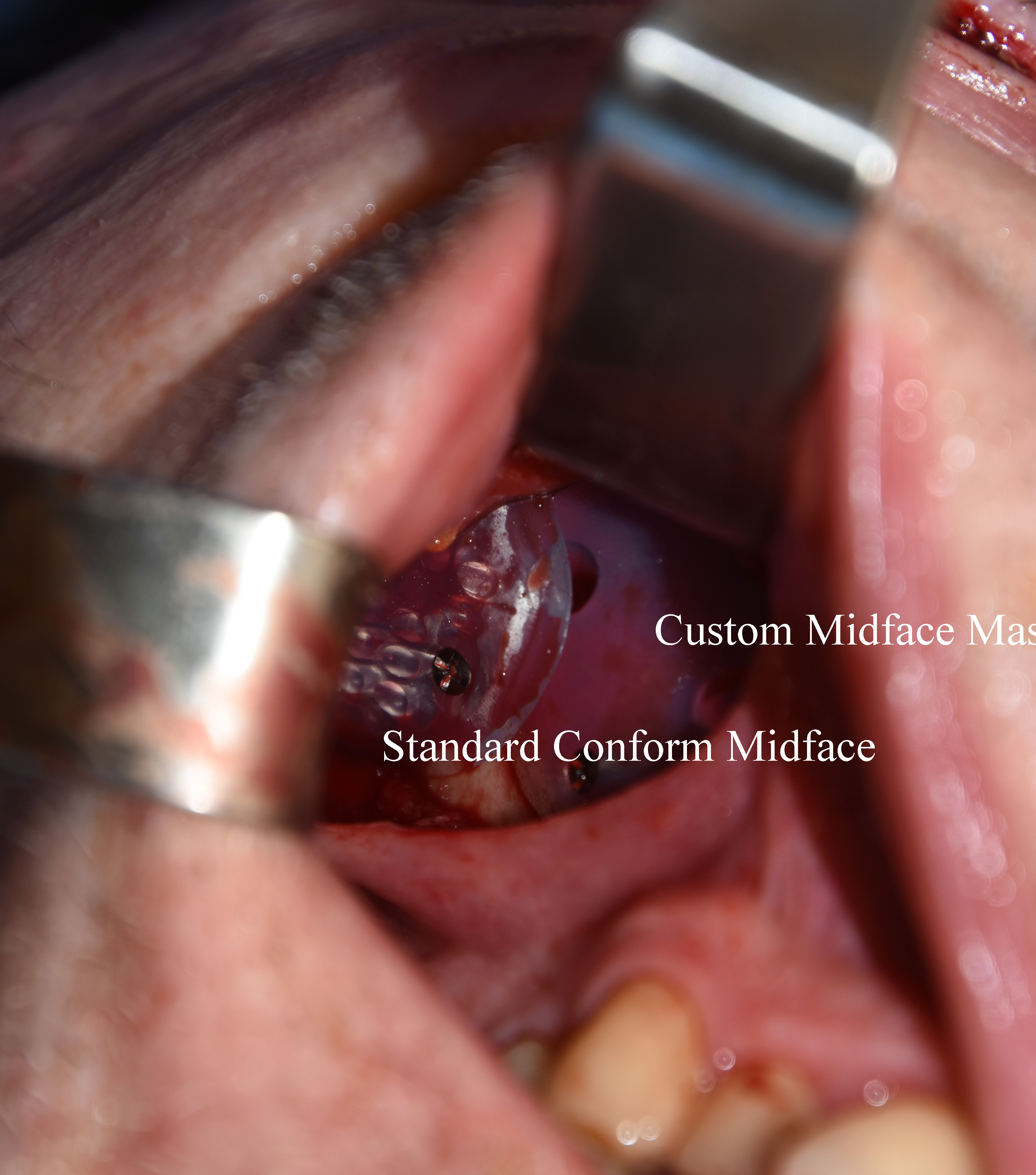 While providing a substance midface augmentation effect, its as felt that more volume was needed in the submalar cheek areas. Thus the placement of standard medium Conform cheek implants was added and secured to the custom implant.
While providing a substance midface augmentation effect, its as felt that more volume was needed in the submalar cheek areas. Thus the placement of standard medium Conform cheek implants was added and secured to the custom implant.
The use of facial implants to add facial volume is not new and is a valuable treatment with standard temporal and cheek implant styles. Custom implants offer an improved amount of volume addition due to their increased bony surface coverage areas
Case Highlights:
1) Loss of volume in the face from lipoatrophy often affects the midface the most significantly.
2) While synthetic injectable fillers and fat injections are primary treatment options, they do not work well for everyone.
3) A custom midface implant that covers all bony surfaces of the midface adds significant volume restoration although does not augment all areas of volume loss.
Dr. Barry Eppley
Indianapolis, Indiana