

Background: The equivalent to female breast augmentation in men are pectoral implants. Besides the obvious differences in aesthetic objectives, pectoral implants differ in that they are solid devices that are placed completely in a submuscular position within the confines of the borders of the pectoralis major muscle. This is almost always done through a transaxillary incisional approach.
Like breast implants, pectoral implants can develop the same complications such as implant malposition and size and shape concerns. Choosing the correct pectoral implant style and size is an art form that belies an exact science to it. Most men today want a chest that has a more rectangular shape that adds visible fullness to the sternal border of the muscle as well in the superomedial pole of the chest. Implant projections range from more modest amounts of 2 cms or so up to 3.5 to 4cm.
One indication for pectoral implants is in cases of corrected precuts excavatum. Even in near optimal corrections the chest is often flat and lacks visible muscle definition. The muscle is often underdeveloped and may have a smaller shape due to an aberrant origin along the sternum/ribcage. The use of pectoral implants in asymmetric chests have a high risk of malpositions and magnifying such pre-existing chest asymmetries.
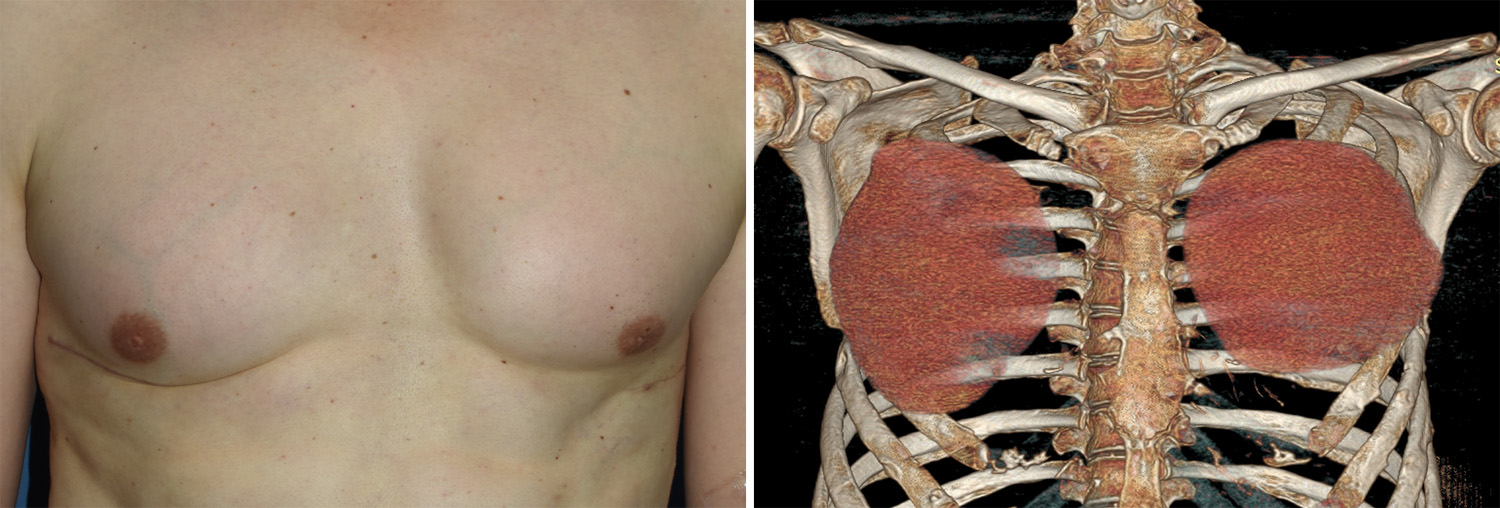 Case Study: This male patient had previously undergone a Nuss procedure for correction of his precuts excavated. This left lateral chest wall scars. He then had pectoral implants placed through these same scars but developed asymmetry in the appearance of is chest. he was uncertain about the exact shape and size of his pectoral implants. A 3D CT scan showed that the right pectoral implant was rotated 90 degrees and was sitting lower as it extended beyond the lateral pectoral muscle border.
Case Study: This male patient had previously undergone a Nuss procedure for correction of his precuts excavated. This left lateral chest wall scars. He then had pectoral implants placed through these same scars but developed asymmetry in the appearance of is chest. he was uncertain about the exact shape and size of his pectoral implants. A 3D CT scan showed that the right pectoral implant was rotated 90 degrees and was sitting lower as it extended beyond the lateral pectoral muscle border.
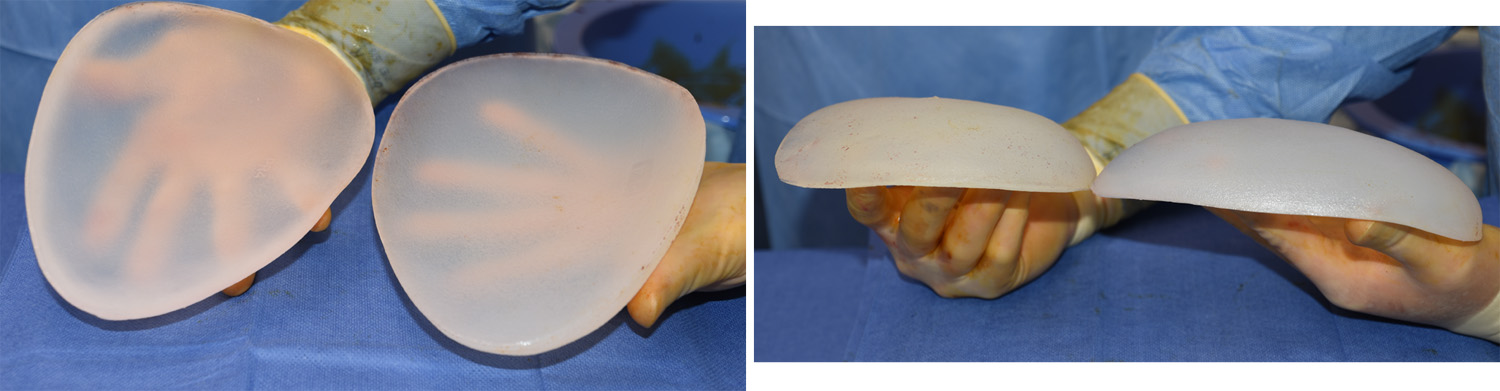
 In considering his pectoral implant replacements, custom implants were designed that had a better shape for his chest but with a similar projection to his indwelling implants.
In considering his pectoral implant replacements, custom implants were designed that had a better shape for his chest but with a similar projection to his indwelling implants.
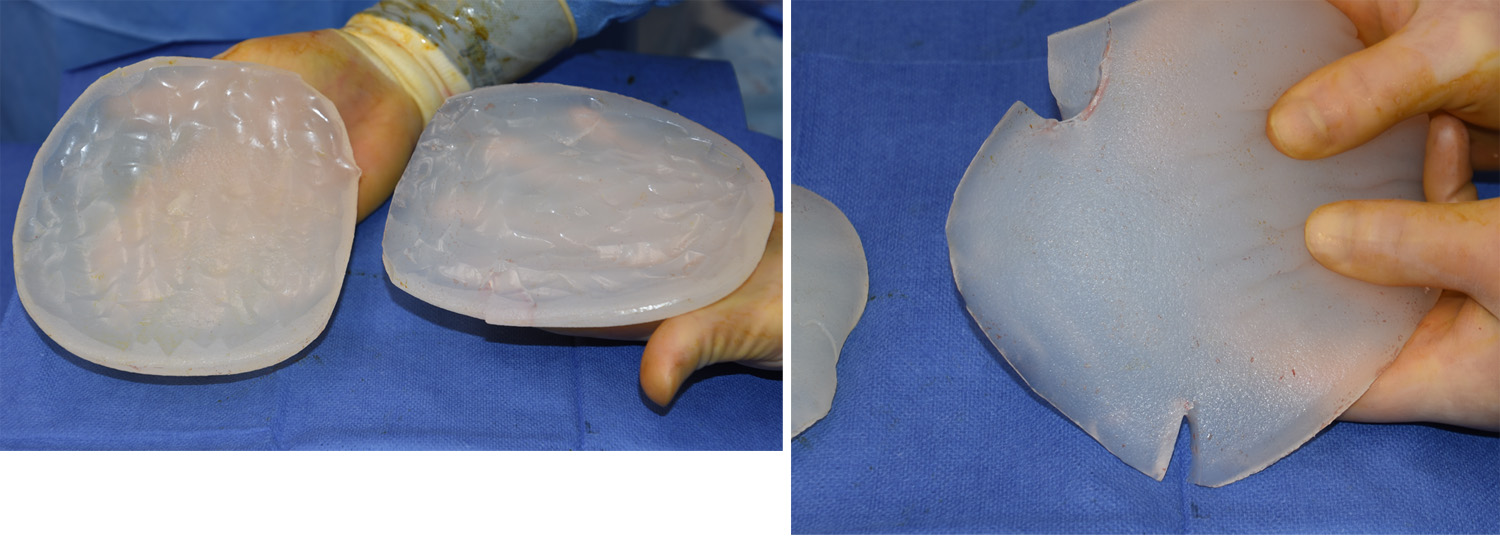
 Under general anesthesia his existing pectoral implants were removed through the lateral chest wall incisions. Both implant pockets had a fluid collection which was greater on the right than the left. The removed implants could be seen to have been modified on their underside and the right implant had tears in two locations. The pockets were cleaned and irrigated and the new implants placed. The lateral border of the right pectoral muscle was re-established/tightened using permanent sutures to the ribcage.
Under general anesthesia his existing pectoral implants were removed through the lateral chest wall incisions. Both implant pockets had a fluid collection which was greater on the right than the left. The removed implants could be seen to have been modified on their underside and the right implant had tears in two locations. The pockets were cleaned and irrigated and the new implants placed. The lateral border of the right pectoral muscle was re-established/tightened using permanent sutures to the ribcage.
This case represents two observations. First, while all solid body implants can be altered, doing so removes the outer shell of the implant exposing the tissues to the sifter inner gel. This can be a potential source for irritation and the development of chronic serums. When possible it is best to not cut into preformed solid body implants. Secondly, custom pectoral implants are ideal when treating chest wall asymmetries that have either been previously implanted or are being treatment planned for the first time.
Highlights:
1) Asymmetry in pectoral implants can be the result of implant positioning or differences in the natural chest anatomy.
2) When in doubt about pectoral implant positioning and style/size, a 3D chest CT scan can help identify the problem.
3) Custom pectoral implants can be an effective solution to chest asymmetry after implant augmentation.
Dr. Barry Eppley
Indianapolis, Indiana