

Background: Soft tissue deformities of the chin are not uncommon and are created by a variety of etiologies. Trauma is the most common cause but developmental chin deformities also occur from hemifacial microsoma and autoimmune diseases from linear scleroderma for example.
Treatment of any soft tissue defects of the face are done by fat injections today. Their ability to introduce a natural soft tissue graft and to do so in a non-incisional method has a lot of appeal. The downside of injectable fat grafting is the unpredictability of its survival or persistence. But the potential need for multiple injection sessions is still worth the lack of creating incisional scars in most cases.
The dermal-fat graft is the original fat grafting procedure that dates back to World War I. Technically the original technique was an enbloc fat graft. (without the dermis) A dermal-fat graft works because the blood vessels are hooked back up quickly within days to a week after implantation. It also helps that fat cells have minimal working parts to them. (just a nucleus) But their success is restricted to smaller graft sizes. Their disadvantages are that they require a donor site harvest and an incision for their placement.
 Case Study: This 45 year-old female suffered a traumatic injury to her chin which resulted in soft tissue atrophy due to the resultant hematoma. The left side of her chin was thinner and had soft tissue contraction and an obvious external deformity. She has some numbness of the mental nerve distribution on that side but a normal working marginal mandibular branch of the facial nerve.
Case Study: This 45 year-old female suffered a traumatic injury to her chin which resulted in soft tissue atrophy due to the resultant hematoma. The left side of her chin was thinner and had soft tissue contraction and an obvious external deformity. She has some numbness of the mental nerve distribution on that side but a normal working marginal mandibular branch of the facial nerve.
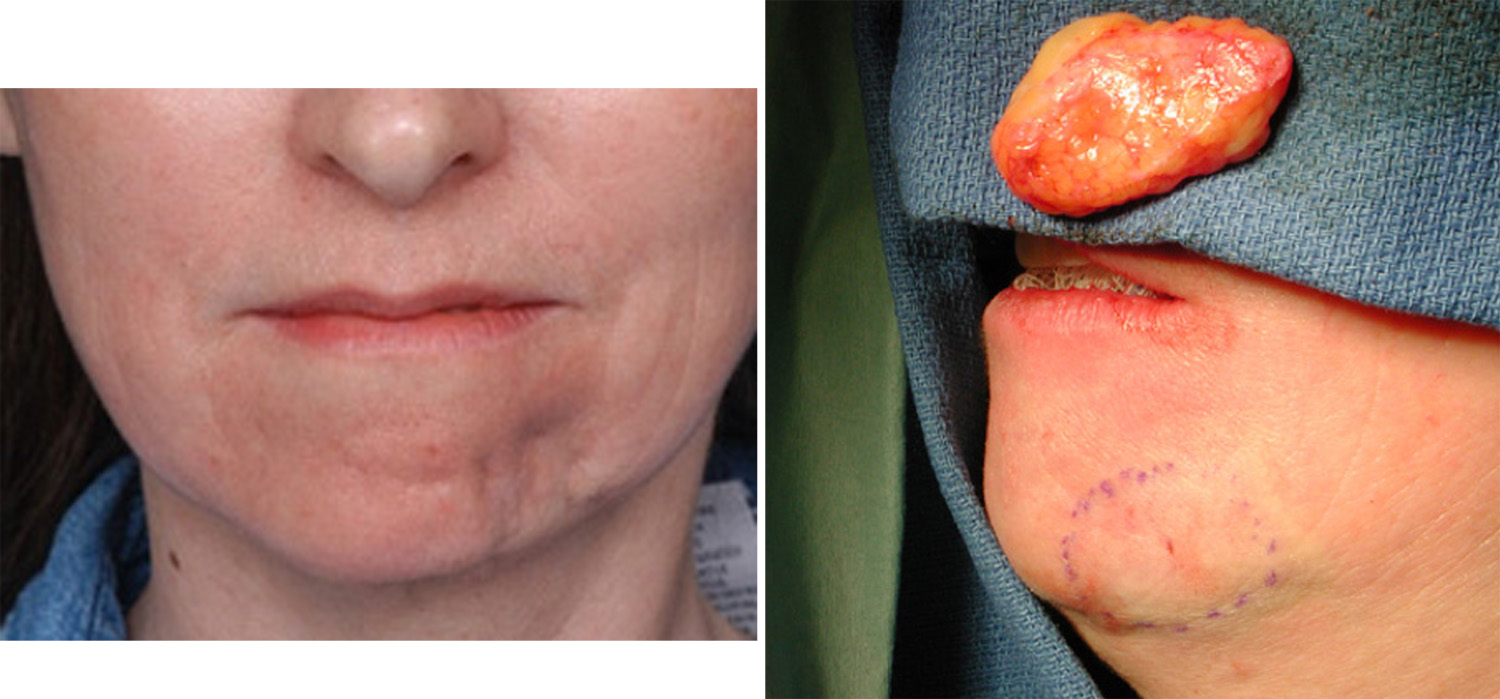 Under general anesthesia, a 4 x 6 cm dermal fat graft was harvested from the lower abdomen. Through an intraoral approach, a vestibular incision made dissecting out branches of the mental nerve. The chin soft tissues were released and a pocket made. The dermal-fat graft was inserted into the pocket and trimmed. A mucosal closure was done over the graft.
Under general anesthesia, a 4 x 6 cm dermal fat graft was harvested from the lower abdomen. Through an intraoral approach, a vestibular incision made dissecting out branches of the mental nerve. The chin soft tissues were released and a pocket made. The dermal-fat graft was inserted into the pocket and trimmed. A mucosal closure was done over the graft.

 Her three month after surgery result showed a near normal chin contour that was fairly soft and supple. No further surgery was required.
Her three month after surgery result showed a near normal chin contour that was fairly soft and supple. No further surgery was required.
The dermal-fat graft is often overlooked in today’s plastic surgery where the injectable fat graft dominates soft tissue reconstruction. While the dermal-fat graft has its limitations, in the properly selected patient it can offer a one-time soft tissue grafting method of reconstruction.
Highlights:
1) Soft tissue deformities of the chin are best treated by fat injections.
2) Fat injections do not always survive and multiple injection sessions may be needed.
3) A dermal-fat graft provides a large soft tissue grafts that can be placed through an intraoral approach with good survival.
Dr. Barry Eppley
Indianapolis, Indiana