

Background: Forehead augmentation or reconstruction is most commonly done using either intraoperatively formed bone cements or a variety of custom designed implant materials. Such forehead implants work best when the overlying scalp tissues are thick and well vascularized. Forehead implant materials should be used with impeding peril when the soft tissue cover is compromised due to injury, resective surgery, or having been treated by radiation.
One well known but uncommon condition that affects the forehead is linear scleroderma. (frontal linear scleroderma) This is a specific form of scleroderma that can affect the forehead and is believed to be an automimmune phenomenon. It presents as an evolving linear band of soft and hard tissue atrophy that usually follows the course of the supraorbital nerve from the brow up into the scalp. It also has atrophic effects below the brow often down through the orbit. Because of its linear indentation appearance up through the forehead it is also known as morphea coup de sabre or ‘cut of the sabre’.
Reconstruction of frontal linear scleroderma has been done by a variety of techniques with the objective of restoring soft tissue thickness. This is usually more important than reconstruction of any bone defect which may exist as it is often a minor part of the forehead contour problem in many cases. Fat injections are the easiest and least invasive method which, while having to be repeated to get optimal take and contour result, do address the thin and atrophic skin which often has little fat underneath. Augmentation with bone cement fills in any bone defect along the linear bone depression but still leaves the soft tissue deficiency if just one alone.
Case Study: This 30 year-old female began to develop linear scleroderma around age 13 and it progressively became worse until it became stable (maximum atrophy) by her early twenties. It involved the left eye, left brow and frontal bone and up into the scalp. A 3D CT scan showed that there was brow bone and frontal bone retrusion. The overlying soft tissues were very thin and atrophic. The skin was very thin and there was little subcutaneous fat between the skin and the bone. While bony forehead reconstruction was needed using bone cement the thinness of her soft tissues was of concern or using this reconstruction method alone..
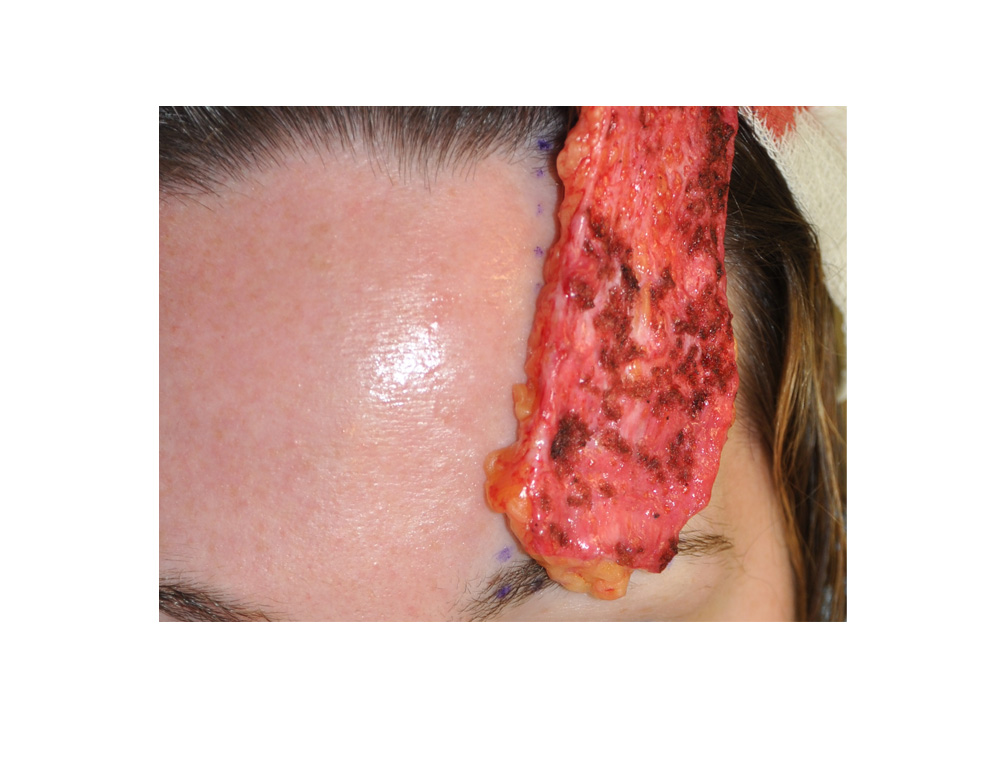
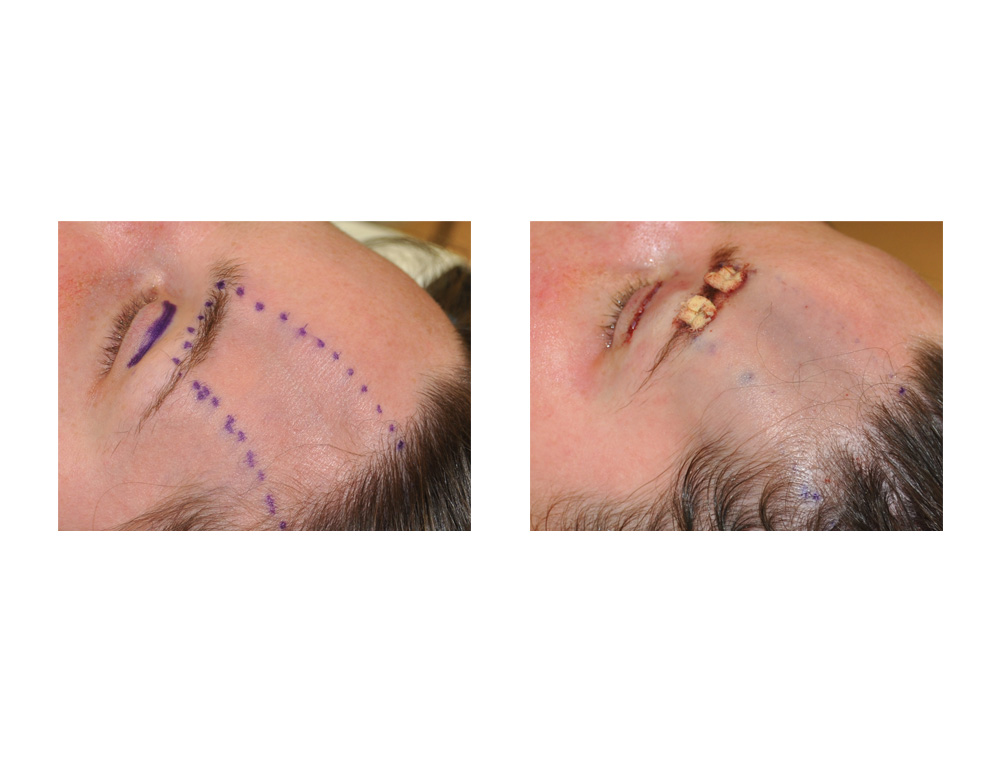 Under general anesthesia, a large dermal-fat graft was harvested from a mini tummy tuck procedure. The overlying epithelium was removed and its thickness trimmed down to approximately one centimeter. Through a small scalp incision directly above the left forehead back in the hairline the dermal fat graft (dermis up) was passed over the bone and secured by external suture bolsters down over the brow bone aided by an upper blepharoplasty incision.
Under general anesthesia, a large dermal-fat graft was harvested from a mini tummy tuck procedure. The overlying epithelium was removed and its thickness trimmed down to approximately one centimeter. Through a small scalp incision directly above the left forehead back in the hairline the dermal fat graft (dermis up) was passed over the bone and secured by external suture bolsters down over the brow bone aided by an upper blepharoplasty incision.
 At one year after the procedure the improvement in the brow and forehead area was very evident with thicker overlying soft tissues and improved brow and forehead contour. This now makes the use of hydroxyapatite cement potentially less problematic with healthier overlying soft tissues.
At one year after the procedure the improvement in the brow and forehead area was very evident with thicker overlying soft tissues and improved brow and forehead contour. This now makes the use of hydroxyapatite cement potentially less problematic with healthier overlying soft tissues.
Dermal-fat grafts are the oldest method of fat grafting and have been over shadowed (and sometimes forgotten) with newer methods of injectable fat grafting. Their biggest drawback is that they require an open excision and resultant scar to harvest and an incision to place them. One also has to have an adequate donor area from which they can be harvested. This is easier in women in large dermal fat grafts with some form of a tummy tuck than it is in men.
Highlights:
1) Forehead augmentation/reconstruction in forehead asymmetry can be done by bone cements or fat grafting.
2) Fat grafting forehead augmentation is best done in pathologic conditions where the forehead skin/tissues are thin.
3) Fat grafting in the forehead can be done by either injection or a dermal-fat graft method.
Dr. Barry Eppley
Indianapolis, Indiana