

Background
Brow bone reduction is a common component of facial feminization surgery (FFS) for the upper third of the face. Because the forehead is a highly gender-defining feature, many transfeminine patients undergo forehead-brow bone reduction, most often with the Type 3 (bone flap) technique. This approach allows for significant brow bone setback by removing and repositioning the outer table of overly convex bone into the frontal sinus, thereby reducing the sinus air space. In some cases, this method can achieve up to 6–8 mm of reduction.
By contrast, the Type 1 brow bone reduction technique leaves the frontal sinus cover intact and reduces prominence by burring or shaving down the bone. This method is more limited in effect, usually allowing for 2–3 mm of reduction, as the thickness of the sinus bone determines how much can safely be removed without exposing the sinus cavity.
The frontal sinuses play a decisive role in brow bone reduction. They are paired structures but are rarely symmetric. A bony septum separates them, often deviating from the midline, which contributes to asymmetry. While frontal sinuses may sometimes be absent or very small, these variations rarely present with prominent brow protrusions of aesthetic concern. Importantly, because of natural asymmetries, it is possible that one side may require a Type 3 technique while the other can be treated with a Type 1 approach.
Case Study
A transfeminine patient presented for forehead feminization, seeking both brow bone reduction and a brow lift through a frontal hairline incision. Although her brow bones were prominent and masculine in appearance, no obvious external asymmetry was noted.

 Under general anesthesia, the bony forehead and brow bones were exposed via a frontal hairline incision extending to the upper temporal region. A reciprocating saw was then used to remove the brow bone prominence by cutting flush with the upper forehead, and an osteotome was employed to complete the bone removal.
Under general anesthesia, the bony forehead and brow bones were exposed via a frontal hairline incision extending to the upper temporal region. A reciprocating saw was then used to remove the brow bone prominence by cutting flush with the upper forehead, and an osteotome was employed to complete the bone removal.

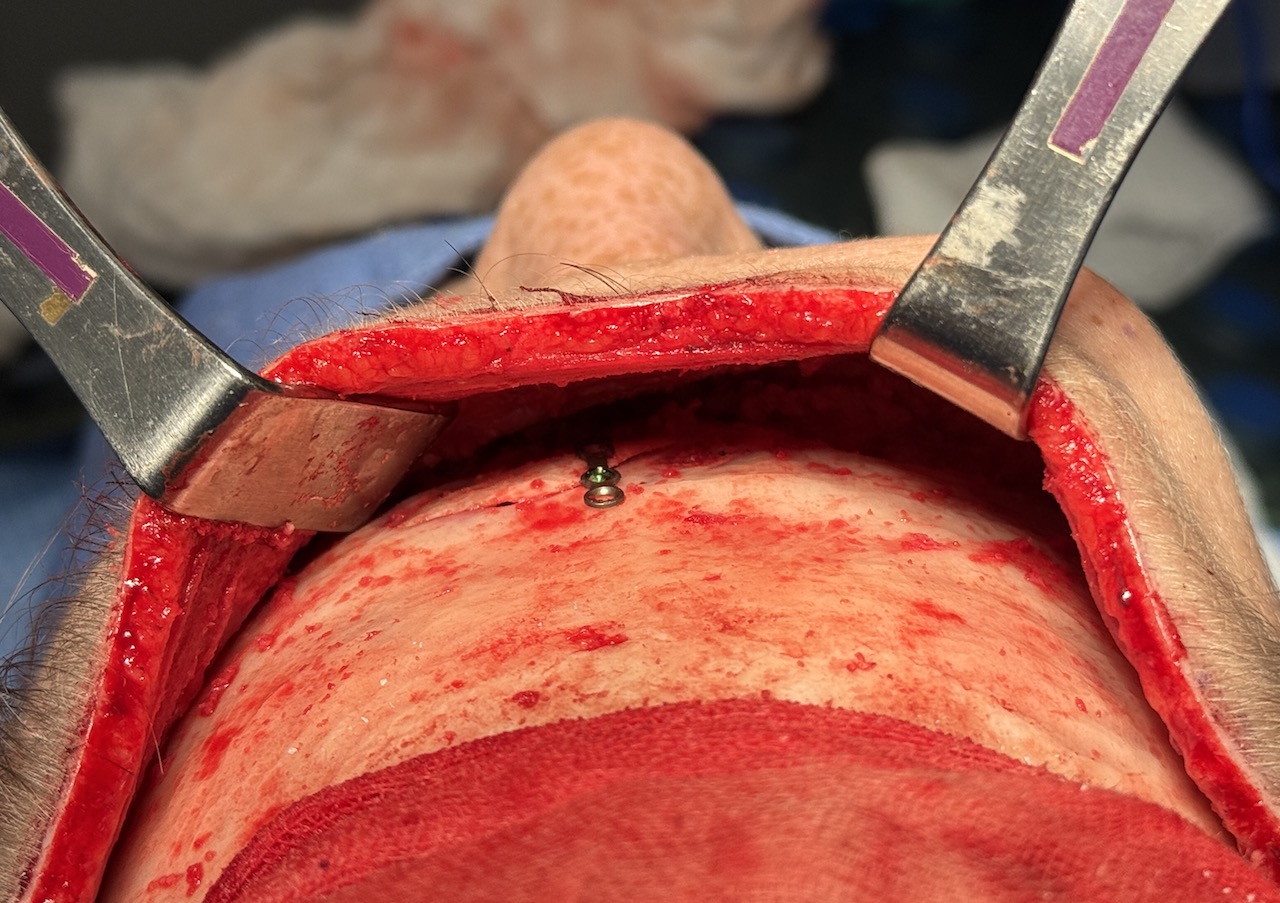
 On the left side, removal of the bone flap exposed the frontal sinus, consistent with a Type 3 technique. On the right side, however, a layer of bone persisted over the sinus, necessitating a Type 1 reduction with further burring. The left bone flap was reshaped and reattached with a single plate fixation. Despite the differing approaches, both brow bones were successfully reduced to a symmetric appearance.
On the left side, removal of the bone flap exposed the frontal sinus, consistent with a Type 3 technique. On the right side, however, a layer of bone persisted over the sinus, necessitating a Type 1 reduction with further burring. The left bone flap was reshaped and reattached with a single plate fixation. Despite the differing approaches, both brow bones were successfully reduced to a symmetric appearance.
 After completing the reduction, a direct brow lift was performed.
After completing the reduction, a direct brow lift was performed.
![]()
![]() The postoperative profile immediately revealed a more feminine forehead contour.
The postoperative profile immediately revealed a more feminine forehead contour.
Discussion
This case highlights an important point: while external brow bone symmetry may be present, the underlying frontal sinus anatomy may be asymmetric. Such internal variations can dictate different surgical strategies on each side. In this case, one side required a bone flap (Type 3) while the other only needed burring (Type 1), underscoring the tailored nature of brow bone reduction.
Key Points
-
The size and bone thickness of the frontal sinus largely determine which brow bone reduction technique is appropriate.
-
Frontal sinus asymmetry is common and does not always correlate with external brow bone shape.
-
In this case, both Type 1 and Type 3 techniques were applied to achieve symmetric results despite differing internal anatomy.
Dr. Barry Eppley
World-Renowned Plastic Surgeon