

Background: The classic debate, and sometimes an actual controversy, is whether chin augmentation is best done with an implant or by moving the chin bone. (sliding genioplasty) While patients and surgeons often try and compare them by their level of invasiveness, that is really an irrelevant and short-sighted thought process to that decision. That discussion more likely emanates from what the surgeon is capable of doing or what the patient may be willing to undergo that what may actually be dimensionally better for the chin deficiency problem.
There are, however, limits as to what either chin augmentation method can accomplish. The largest standard chin implants can provide no more than 11mms of horizontal projection, very little if any vertical increase (1 to 2mms) and variable amounts of width. (although I have made custom chin implants with as much as 17mms of horizontal width and 10mms of vertical length and variables amounts of increased chin widths) Conversely a sliding genioplasty offers different dimensional possibilities with horizontal increases up to 16mms (based on the patient’s thickness of bone), 10mms of vertical lengthening through am opening wedge but no real width change possibilities as an intact down fractured bone segment.
Extreme chin augmentation is defined, by my definition, when the dimensional changes needed exceed whatever is possible using standard performed chin implants or within the bony contact limits of a sliding genioplasty. As a result extreme chin augmentation requires either combining an implant with a sliding genioplasty or the fabrication of a custom chin implant.
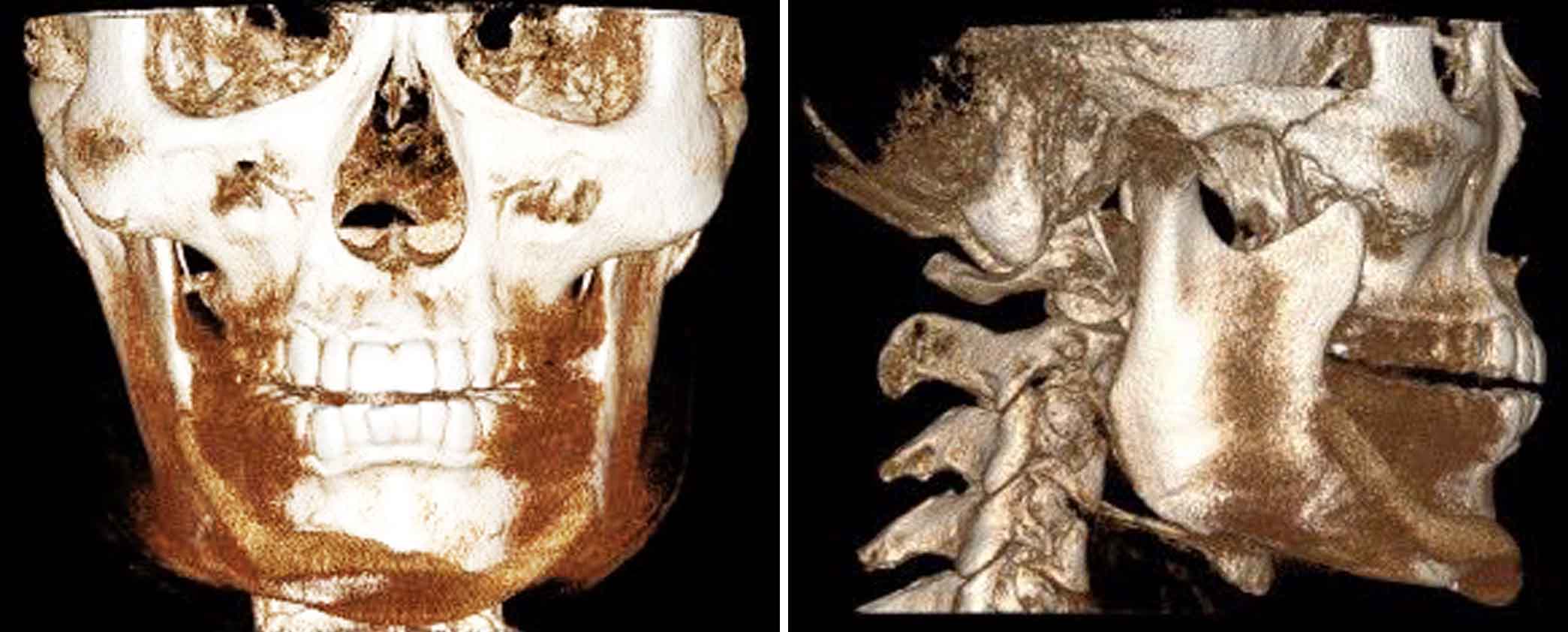 Case Study: This young male had an indwelling chin implant to treat his significant aesthetic chin deficiency. While providing improvement at 11mms of increased horizontal projection it remained deficient in both the horizontal and vertical dimensions. In addition a 3D CT scan showed that there was significant asymmetrical placement as well. Through computer imaging and patient and patient measurements it was determined that he needed another 5mms of horizontal projection and as well as a 4 to 5mm vertical increase as well.
Case Study: This young male had an indwelling chin implant to treat his significant aesthetic chin deficiency. While providing improvement at 11mms of increased horizontal projection it remained deficient in both the horizontal and vertical dimensions. In addition a 3D CT scan showed that there was significant asymmetrical placement as well. Through computer imaging and patient and patient measurements it was determined that he needed another 5mms of horizontal projection and as well as a 4 to 5mm vertical increase as well.
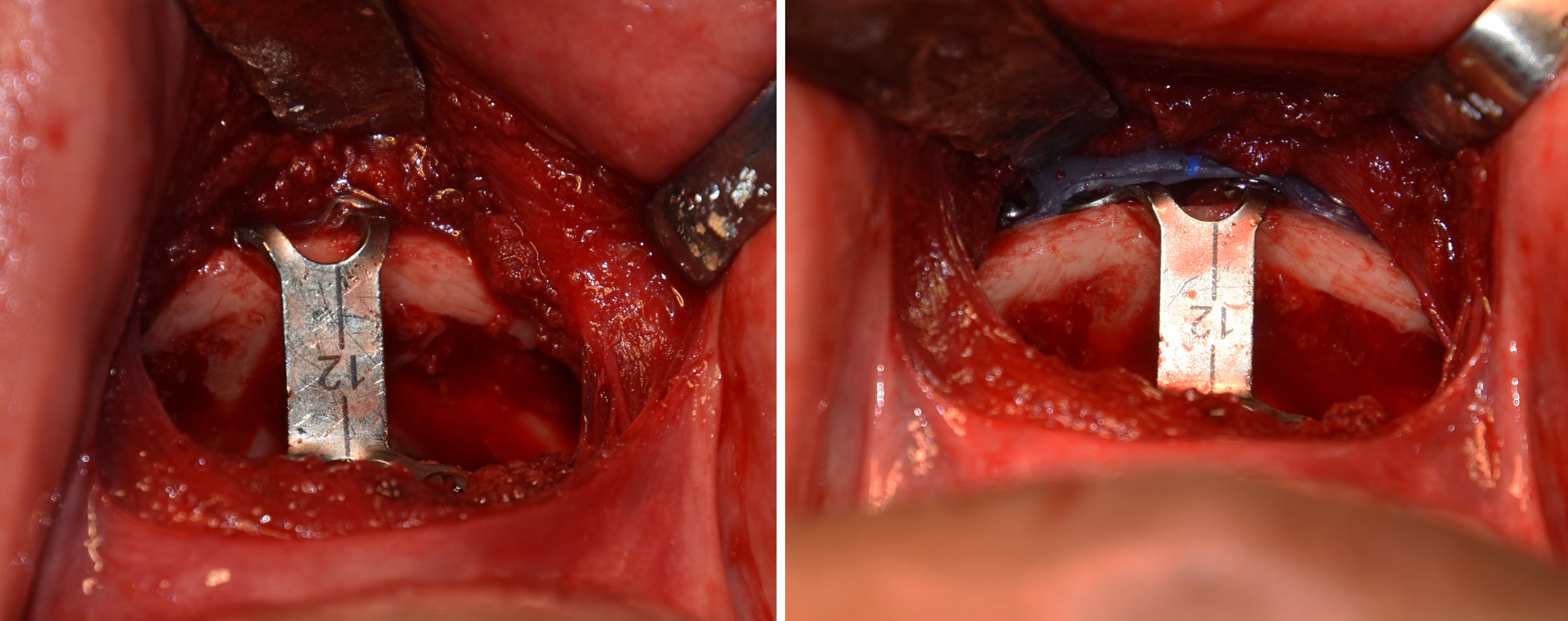
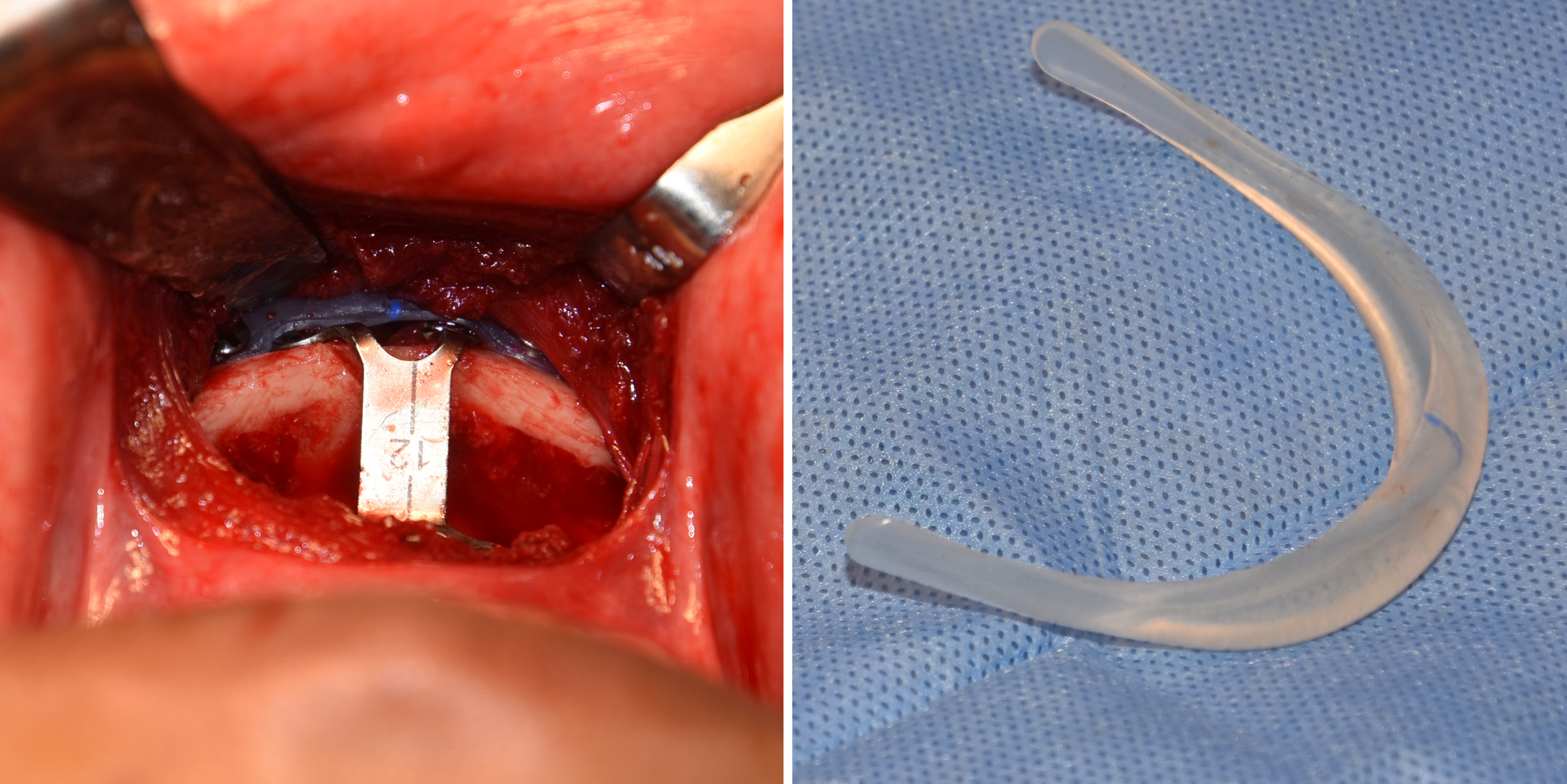 Under general anesthesia and through an intraoral approach, the indwelling chin implant was removed. A slightly angled horizontal bone cut was made running back 40mms from the midline and 5mms below the mental foramen. The down fractured chin bone was moved out 12mms and down 4mms and secured with an angled step titanium chin plate and screws. A more rigid chin-prejowl implant of 5mms thickness was placed as an overlay on the front edge of the chin with the wings extending back over the bony step offs of the distal tail of the sliding genioplasty. This provide both the additional amount of horizontal augmentation needed as well as camouflage for the potentially palpable bony irregularities that commonly occur from a sliding genioplasty.
Under general anesthesia and through an intraoral approach, the indwelling chin implant was removed. A slightly angled horizontal bone cut was made running back 40mms from the midline and 5mms below the mental foramen. The down fractured chin bone was moved out 12mms and down 4mms and secured with an angled step titanium chin plate and screws. A more rigid chin-prejowl implant of 5mms thickness was placed as an overlay on the front edge of the chin with the wings extending back over the bony step offs of the distal tail of the sliding genioplasty. This provide both the additional amount of horizontal augmentation needed as well as camouflage for the potentially palpable bony irregularities that commonly occur from a sliding genioplasty.
While a sliding genioplasty and a chin implant are typically perceived as completely independent procedures, there is no biologic reason they can not be combined if the patient’s dimensional needs so require. Having done such combination chin surgeries over twenty times in the past two decades it has not shown any increased risks of complications behind what whether procedure alone has. The key is to make the sliding genioplasty the workhorse of the procedure to keep the ‘implant load’ low.
Highlights:
1) Both chin implants and sliding geniplasties have limits for how much horizontal projection they can provide.
2) The combination of a sliding genioplasty and an overlay chin implant can create greater dimensional changes that either one can alone. (extreme chin augmentation)
3) Having an indwelling chin implant is helpful in extreme chin augmentation because it creates some existing stretch of the soft tissue chin pad.
Dr. Barry Eppley
Indianapolis, Indiana