

Background: Lip rejuvenation is most commonly done by injectable fillers. By adding internal volume the lip gets bigger and, most of the time, looks more aesthetically appealing. But injectable fillers will not work for all aesthetic lip concerns. It can not reduce the amount of skin in the upper lip nor can it increase the amount of tooth show. Should these features of the upper lip need to be improved, an excisional approach is needed.
Excisional lip procedures involve the removal of skin to create their effects. This can be done either under the nose (lip lift) or from just above the upper lip line. (lip advancement) There are specific indications for either excisional lip procedure and they are often confused. Fundamentally, a lip lift only changes the central portion of the upper lip while a lip advancement changes the entire vermilion appearance of the whole lip form corner to corner. Both shorten the vertical length of skin of the upper lip and may improve tooth show. A lip lift accentuates the current shape of the cupid’s bow while a lip advancement can dramatically change the shape of it. The different location of the resultant lip scars are also obviously different.
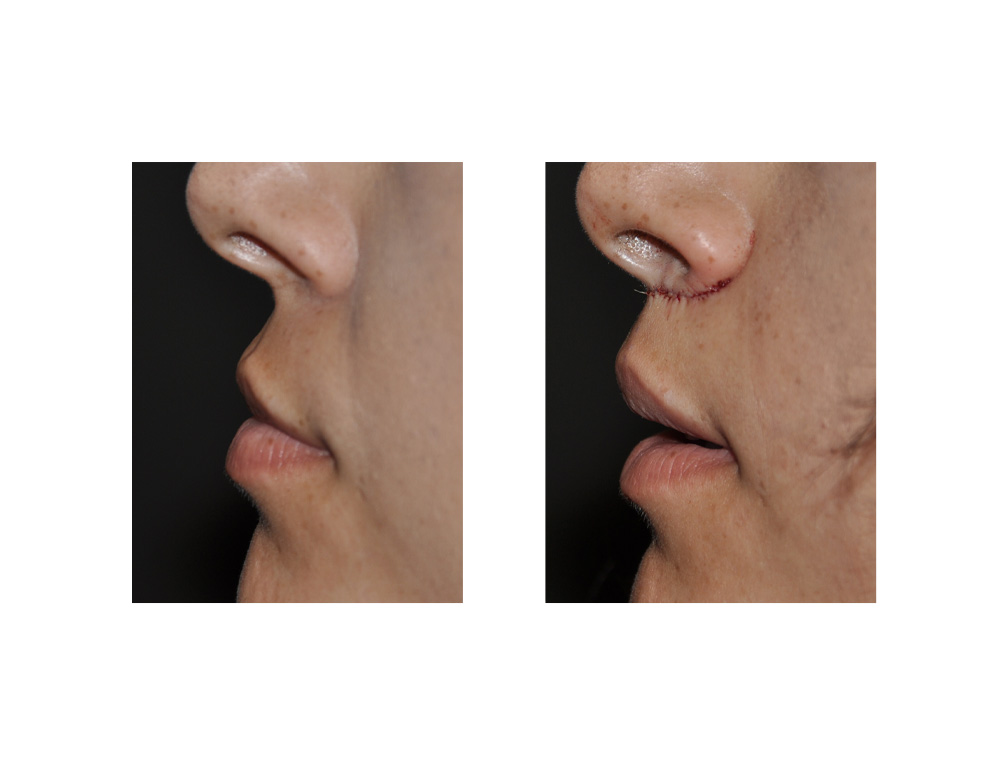
Case Study: This 26 year-old Hispanic felt that her upper lip was too long and she did not have enough tooth show. She has very reasonable vermilion shape and fullness but she was not opposed to a more pronounced cupid’s bow appearance. She had tried injectable fillers but this did not give her the upper lip look she was seeking.
 An irregular wavy line excision pattern was marked out under the nose in what is often called a ‘bullhorn’ shape. The maximal width of the excision was marked out along the philtral columns based on a preoperative measurement of 15.5mm length with a 5mm skin excision along these lines) The marked excision pattern tapered into the crease at the sides of the nostrils. Under local anesthesia (infraorbital nerve blocks with direct infiltration), the intervening skin segments were excised in two pieces exposing the orbicularis muscle. The lip segments was lifted and sewn in a two-layer closure with resorbable sutures. Antibiotic ointment was applied as the only dressing.
An irregular wavy line excision pattern was marked out under the nose in what is often called a ‘bullhorn’ shape. The maximal width of the excision was marked out along the philtral columns based on a preoperative measurement of 15.5mm length with a 5mm skin excision along these lines) The marked excision pattern tapered into the crease at the sides of the nostrils. Under local anesthesia (infraorbital nerve blocks with direct infiltration), the intervening skin segments were excised in two pieces exposing the orbicularis muscle. The lip segments was lifted and sewn in a two-layer closure with resorbable sutures. Antibiotic ointment was applied as the only dressing.
 The results from a subnasal lip lift are immediate as one would expect from the vertical skin shortening. While the upper lip is moved upward to be closed under the nose. There can be a slight pulling down of the base of the nose in some cases. This has led to some surgeons doing deep sutures, sewing either the muscle or the dermis of the advanced upper lip skin flap to the anterior nasal spine. This well-intentioned suture manuever is ill-advised as it can affect how the upper lip moves or cause other distortions.
The results from a subnasal lip lift are immediate as one would expect from the vertical skin shortening. While the upper lip is moved upward to be closed under the nose. There can be a slight pulling down of the base of the nose in some cases. This has led to some surgeons doing deep sutures, sewing either the muscle or the dermis of the advanced upper lip skin flap to the anterior nasal spine. This well-intentioned suture manuever is ill-advised as it can affect how the upper lip moves or cause other distortions.
 As long as not too much skin is removed from the upper lip (never more than 1/3), this slight pulling down effect is temporary and is not of an aesthetic concern. All subnasal lip lifts will eventually suffer some relapse of up to 20% of the skin removed, that is a far easier problem to correct if desired than any type of lip distortion caused by muscle manipulation or deep suturing manuvers.
As long as not too much skin is removed from the upper lip (never more than 1/3), this slight pulling down effect is temporary and is not of an aesthetic concern. All subnasal lip lifts will eventually suffer some relapse of up to 20% of the skin removed, that is a far easier problem to correct if desired than any type of lip distortion caused by muscle manipulation or deep suturing manuvers.
Case Highlights:
1) A subnasal lip lift is an effective lip enhancement procedure whose effects are limited to the central portion of the upper lip. (cupid’s bow)
2) A subnasal lip lift will shorten the upper lip with a minimal effect on increasing upper tooth show.
3) A subnasal lip lift should not remove than one-third of the vertical skin distance between the nose and the lip and should never remove or plicate the orbicularis muscle.
Dr. Barry Eppley
Indianapolis, Indiana