

Background: The shape of the eye has a significant impact on both facial appearance and expression. Its inner and outer shape is largely created by the overlying eyelids and how they come together and attach to the inside and outside of the orbital bones. The union of the upper and lower eyelids forms the inner and outer corners and this union also creates the aperture or angle between eye corners. The outside corner of the eye is probably the more important half since it controls the horizontal orientation of how eye shape is perceived.
Eye shape most commonly has a neutral axis or a completely horizontal orientation. This means that the inner and outer eye corners are at the same horizontal spot on the orbital rim bones which creates a straight line across the eye when drawn between the two. A downward eye tilt means that the outer corner is lower than the inner corner. Conversely, an upward tilt to eye shape means that the outer corner is higher than the inner.
A horizontal or upward tilt to the outer corner of the eye is seen as most desired. Some women even prefer a more exaggerated or exotic eye cant with the outer corner being much higher than the inner corner. A downward eye tilt, which some people have naturally, is seen as undesired and can also occur from loss of outer corner lid support from any type of lower eyelid surgery.
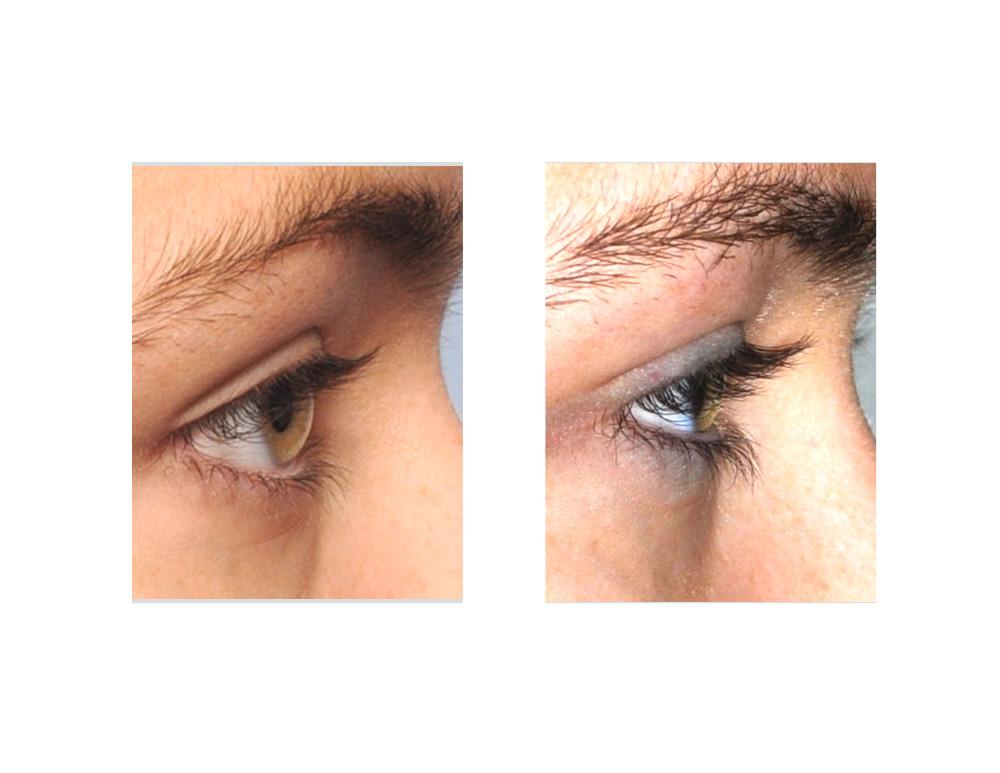
Case Study: This 22 year-old female wanted to change the outer corner of her eyes slightly to fix their asymmetry and eliminate excessive scleral show. This was her natural eye shape and eyelid position.
 Because she was having numerous other cosmetic procedures, her surgery was done under general anesthesia. Through a 7mm skin incision in the outer skin crease, lateral canthopexies were performed. The outer corners of the eye were sutured up higher on the outer aspect of the lateral orbital rims with small permanent sutures. The skin incisions were closed with very small resorbable sutures. Her six month after surgery pictures show the sustained improvement in her lower eyelid outer corner repositioning.
Because she was having numerous other cosmetic procedures, her surgery was done under general anesthesia. Through a 7mm skin incision in the outer skin crease, lateral canthopexies were performed. The outer corners of the eye were sutured up higher on the outer aspect of the lateral orbital rims with small permanent sutures. The skin incisions were closed with very small resorbable sutures. Her six month after surgery pictures show the sustained improvement in her lower eyelid outer corner repositioning.

 Lateral canthopexies can elevate the outer corner of the eye and can do so without creating a bowstring or tightening effect across the entire lower eyelid. Because it stays on the outside of the bone (rather than inside like a lateral canthoplasty) it does not shorten the horizontal length of the lower eyelid. In addition, it helps to correct prevent rounding of eye shape which is more associated with that of an aging look.
Lateral canthopexies can elevate the outer corner of the eye and can do so without creating a bowstring or tightening effect across the entire lower eyelid. Because it stays on the outside of the bone (rather than inside like a lateral canthoplasty) it does not shorten the horizontal length of the lower eyelid. In addition, it helps to correct prevent rounding of eye shape which is more associated with that of an aging look.
Case Highlights:
1) Improving the upward tilt of the corners of the eyes can be done by either lateral canthopexy or lateral canthoplasty techniques.
2) Lateral canthopexy vs. canthoplasty have different impacts of eye shape.
3) A lateral canthopexy technique is less likely to round out the eye shape and shorten the horizontal length of the lower eyelid.
Dr. Barry Eppley
Indianapolis, Indiana