

Background: Ptosis or structural sagging is known to affect many body areas, most commonly that of the breasts for which a classification scheme has been devised for it to help with treatment strategies for its correction. But sagging also affects the buttocks and is fairly well recognized. It most commonly develops as a result of weight loss but can also occur from aging and is more prone in thinner people.
Buttock ptosis comes in two types based on the location of the infragluteal crease. Type I buttock ptosis is where the infragluteal fold is at a good location but the lower end of the buttock tissues have fallen over it. This is also known as a banana roll and attempts to treat it often involve liposuction…which usually fails to provide the desired improvement. Type II buttock ptosis is where the infragluteal fold has actually fallen or lowered. (bottomed out) This lengthens the buttock but the tissues do not fall over the fold because of its lower position.
The definitive treatment of buttock ptosis is an excisional one. In type 1 ptosis the overhanging tissue is removed and the infragluteal crease is maintained where it is. In type II ptosis tissue excised but a new and higher level of the fold is created.
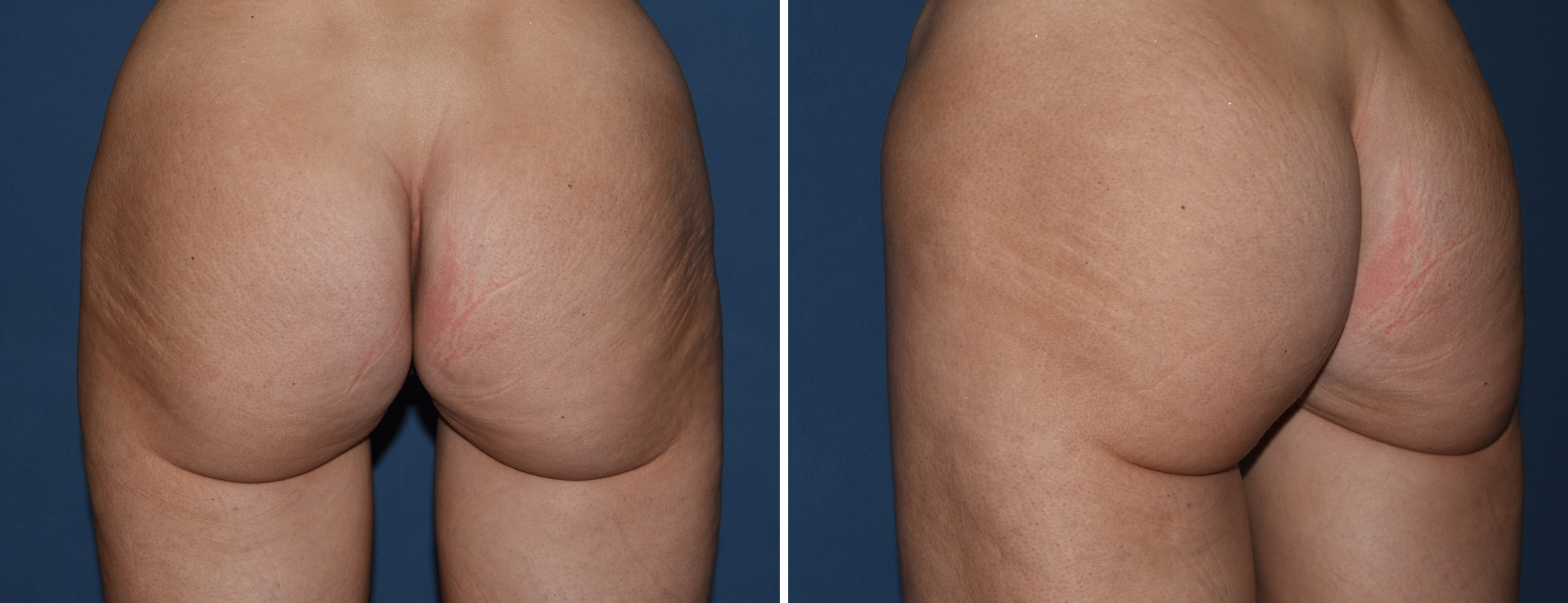
 Case Study: This female presented with concerns about buttock ‘drooping’ and a vertically long buttocks. She had a history of some weight loss. The markings for the buttock lift included the excision pattern which must be done at least 1 cm above the current fold level so that closure results in a higher infragluteal fold location in a type II buttock ptosis repair.
Case Study: This female presented with concerns about buttock ‘drooping’ and a vertically long buttocks. She had a history of some weight loss. The markings for the buttock lift included the excision pattern which must be done at least 1 cm above the current fold level so that closure results in a higher infragluteal fold location in a type II buttock ptosis repair.
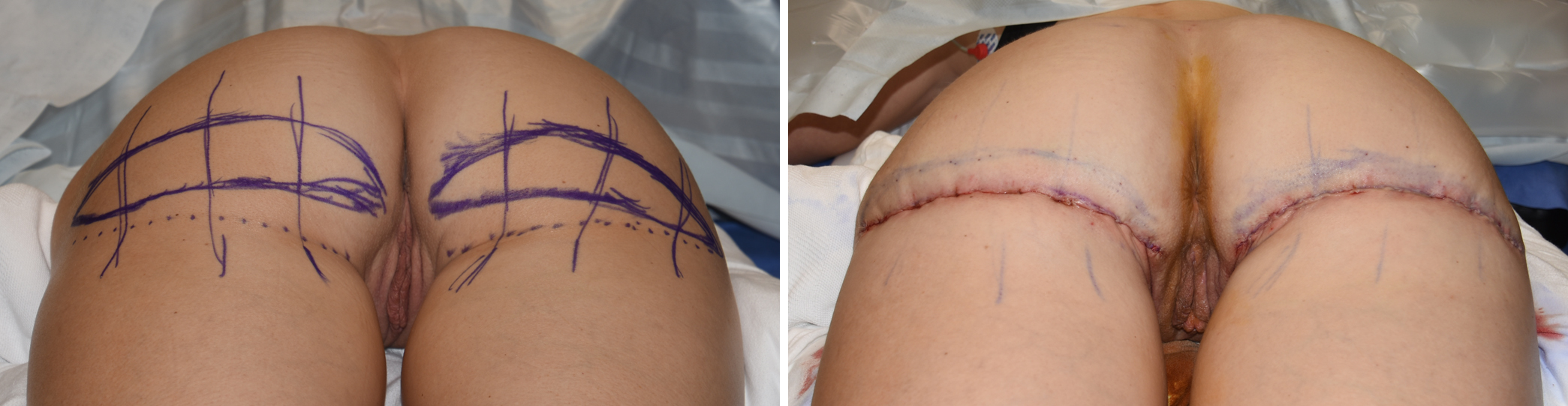
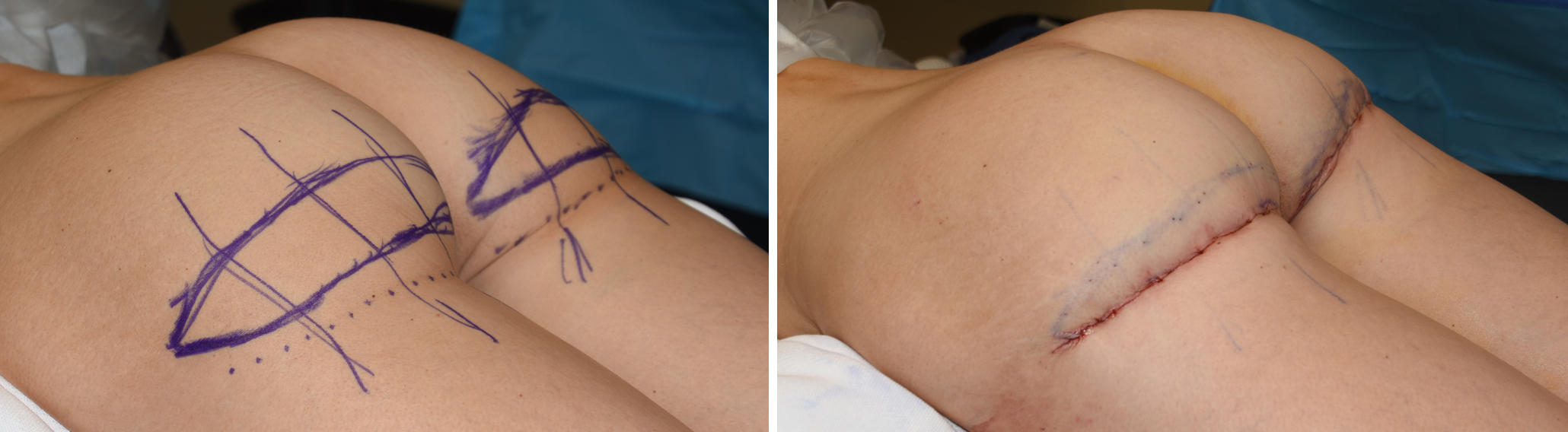 Under general anesthesia and in the prone position, the skin was incised along the marks and a small wedge of fat removed down to the gluteal fascia. Multiple dermal-fascial sutures were placed to recreate the infragluteal fold at a higher level. The skin was closed with a subcuticular suture.
Under general anesthesia and in the prone position, the skin was incised along the marks and a small wedge of fat removed down to the gluteal fascia. Multiple dermal-fascial sutures were placed to recreate the infragluteal fold at a higher level. The skin was closed with a subcuticular suture.

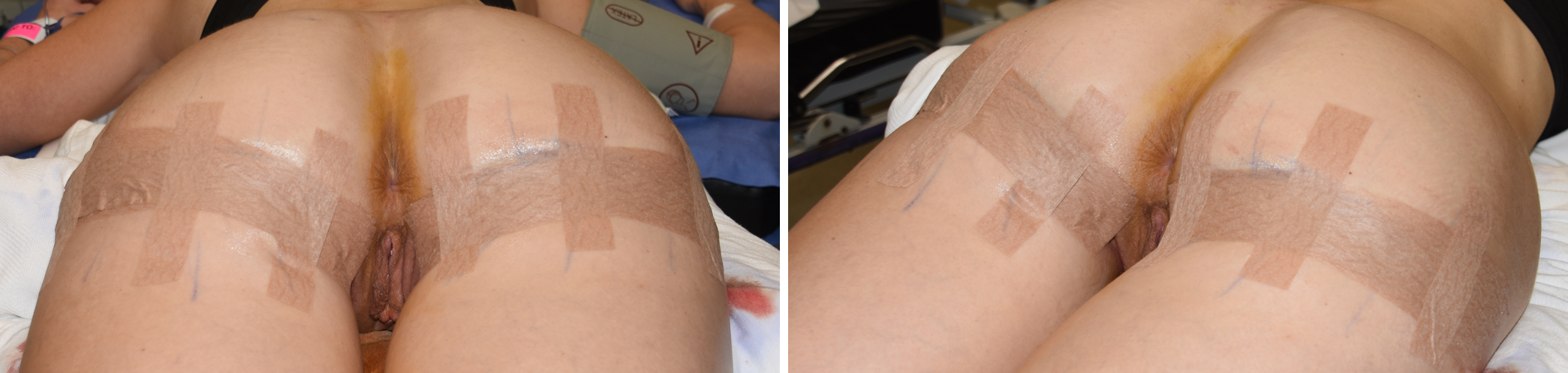 The only dressing used for a lower buttock lift is multiple layers of microporous tapes applied along and across the incisions with skin adhesive.
The only dressing used for a lower buttock lift is multiple layers of microporous tapes applied along and across the incisions with skin adhesive.
A lower buttock lift corrects the ptosis with an exciosnal approach whose location depends on whether the infragluteal fold is maintained or to be elevated.
Highlights:
1) Buttock ptosis must consider the existing location of the infragluteal crease to determine the proper buttock lift technique.
2) With a low infragluteal crease and a long vertical buttock length, the buttock lift must establish a new and higher position for the fold to shorten the buttocks.
3) The location of the skin excision and the use of dermal-fascial suturing are the key elements of all buttock lift techniques.
Dr. Barry Eppley
Indianapolis, Indiana