

Background: The lower eyelid is uniquely different from that of the upper eyelid. Besides being on the lower half of the eyeball, it has much less movement than that of the upper eyelid. The lower eyelid is largely static and is best thought of as a ‘clothesline’ running across the lower half of the eye. Being attached by the canthal tendons to the inside of the eye socket bones on each side, the lower eyelid is held tightly against the eyeball. By being right up against the eyeball, it serves to help keep the eye lubricated and provides a pathway for tear drainage.
Any surgery that involves the lower eyelid always runs the risk of disrupting its intimate and important relationship to the eyeball. While there are different eyelid incisional approaches, all have the potential to cause scarring and retraction pulling the eyelid down and away from the eyeball. (known as ectropion) Besides the obvious adverse aesthetic effects, loss of lid-eyeball contact leads to irritation, dryness and excessive tearing.
Reconstruction of lower eyelid ectropion can be challenging. It is almost never as simple as just ‘releasing the lower eyelid and pulling it back into place’. The lower eyelid layers are scarred and may be now short of supple tissue. Tissue grafting may be needed to overcome the scarred tissues and to prevent the pull down of the lower eyelid from recurring.
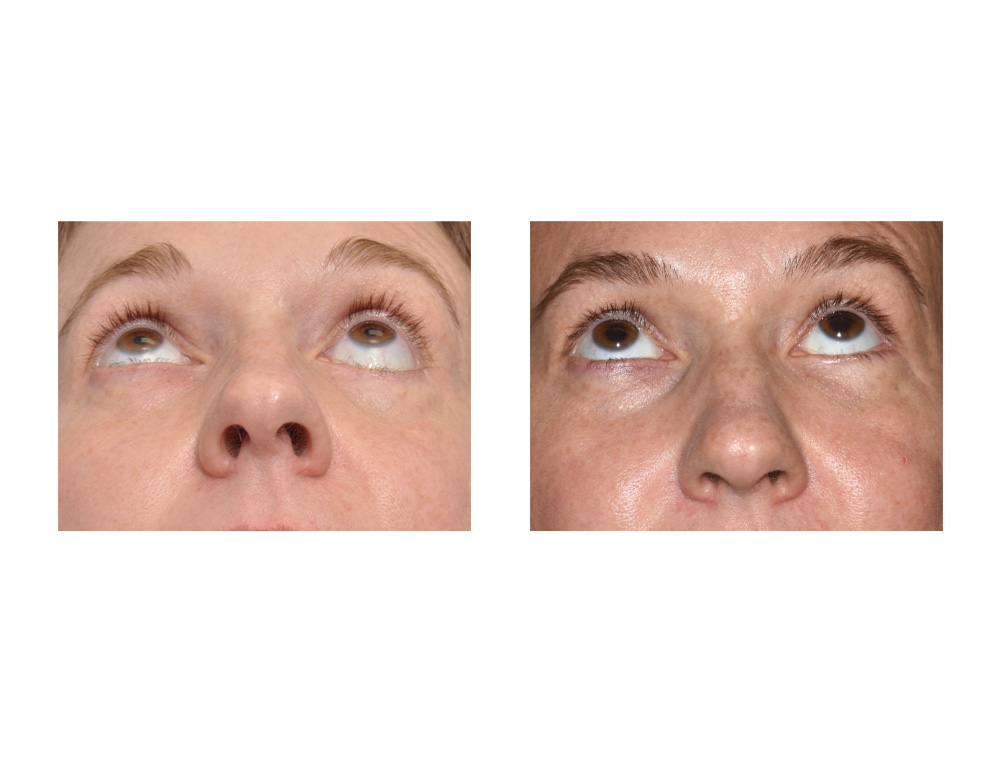
Case Study: This 40 year old female had a prior history of a left cheekbone fracture that was repaired by another surgeon. Six months after her repair the original surgeon removed her plates and screws used to fix the fracture and attempted to fix a lower eyelid ectropion. The eyelid ectropion repair was unsuccessful and actually became worse.

 Under general anesthesia a tranconjunctival and lateral canthal incisional approach was used. The lower eyelid tissues were released of all scar from the infraorbital rim. This created and internal conjunctival lining defect which was grafted with buccal mucosa. A lateral canthoplasty was performed using a double hole technique through the lateral orbital rim. Adjunctive procedures including fat injections to the cheek were also done to built up the tissues below the eyelid for typical fat atrophy that occurs after trauma.
Under general anesthesia a tranconjunctival and lateral canthal incisional approach was used. The lower eyelid tissues were released of all scar from the infraorbital rim. This created and internal conjunctival lining defect which was grafted with buccal mucosa. A lateral canthoplasty was performed using a double hole technique through the lateral orbital rim. Adjunctive procedures including fat injections to the cheek were also done to built up the tissues below the eyelid for typical fat atrophy that occurs after trauma.
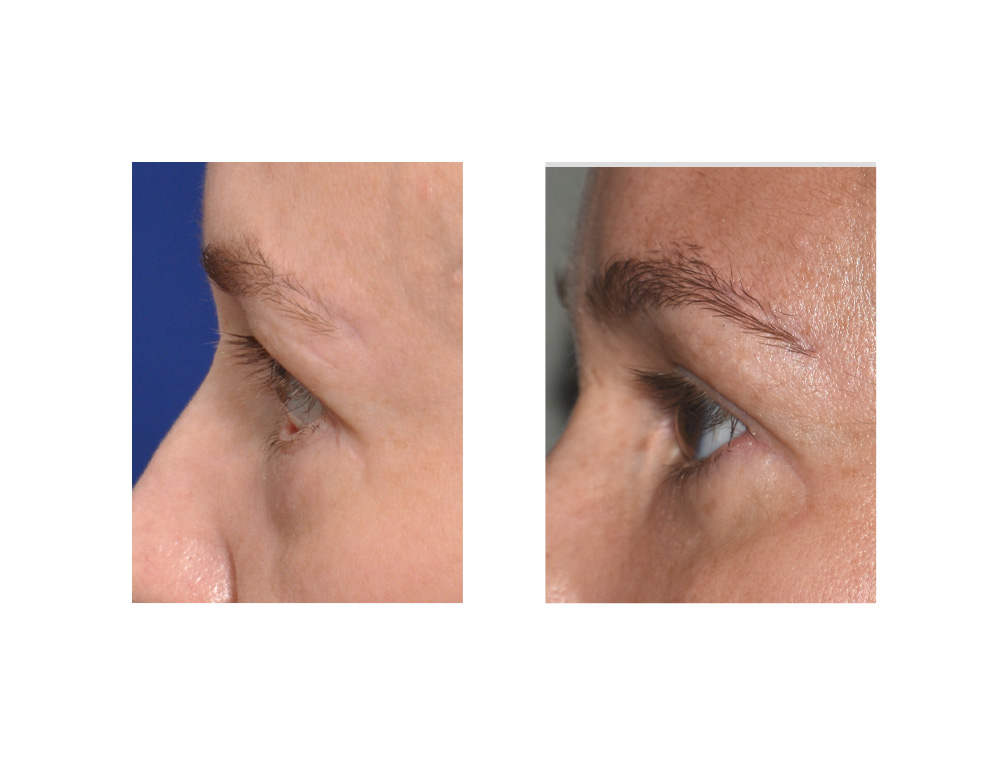 Her 6 months results that she achieved restoration of a competent lower eyelid that relieved all of her eye symptoms. The result is far from perfect as her lateral eyelid aperture ended up being slightly horizontally shorter than the opposite side.
Her 6 months results that she achieved restoration of a competent lower eyelid that relieved all of her eye symptoms. The result is far from perfect as her lateral eyelid aperture ended up being slightly horizontally shorter than the opposite side.
Highlights:
1) Lower eyelid retraction can occur from a variety of surgical endeavors including cosmetic blepharoplasties and orbital and cheek bone fracture repairs.
2) Severe retraction with vertical shortening of the lower eyelid indicates a loss of eyelid lining at one or several lamellar layers.
3) Severe lower eyelid ectropion repair usually requires multiple surgeries with tissue grafting to achieve an improved horizontal lower lid position and good adaptation back against the eyeball.
Dr. Barry Eppley
Indianapolis, Indiana