

Background: Any ear that is vertically longer than 65mm to 70mm would generally be perceived to be very large. Despite the numbers, however, if a patient thinks their ears are too large then they are. But in my experience patients that I see for macrotia reduction always have an ear length that is at least 65mms or greater.
Macrotia reduction is usually a ‘high and low’ procedure. This means that the top and the bottom of the ear are shortened as they offer less scar burden to do so. While one could argue that the middle of the ear is the most effective location to do a vertical ear reduction, the resultant visible scar across the middle of the ear would be considered an aesthetic drawback.
In many macrotia cases the greatest vertical ear reduction comes from shortening the earlobe. This is the only completely soft tissue component of the ear and is the most amenable to the greatest tissue removal. The upper portion of the ear is the other area for vertical eat reduction. Hiding most of the incision under the helical rim allows for a wedge of skin and cartilage to be removed and the height of the ear reduced. It is limited to how much ear cartilage can be removed and have the ear not look deformed. It is not often done alone but can be effective.
Case Study: This 35 year-old male felt his ears were too big. While his vertical ear height was 77mms, his earlobes were very small. He had a large conchal bowl but a middle of the ear macrotia reduction approach was not acceptable due to the potential scar.
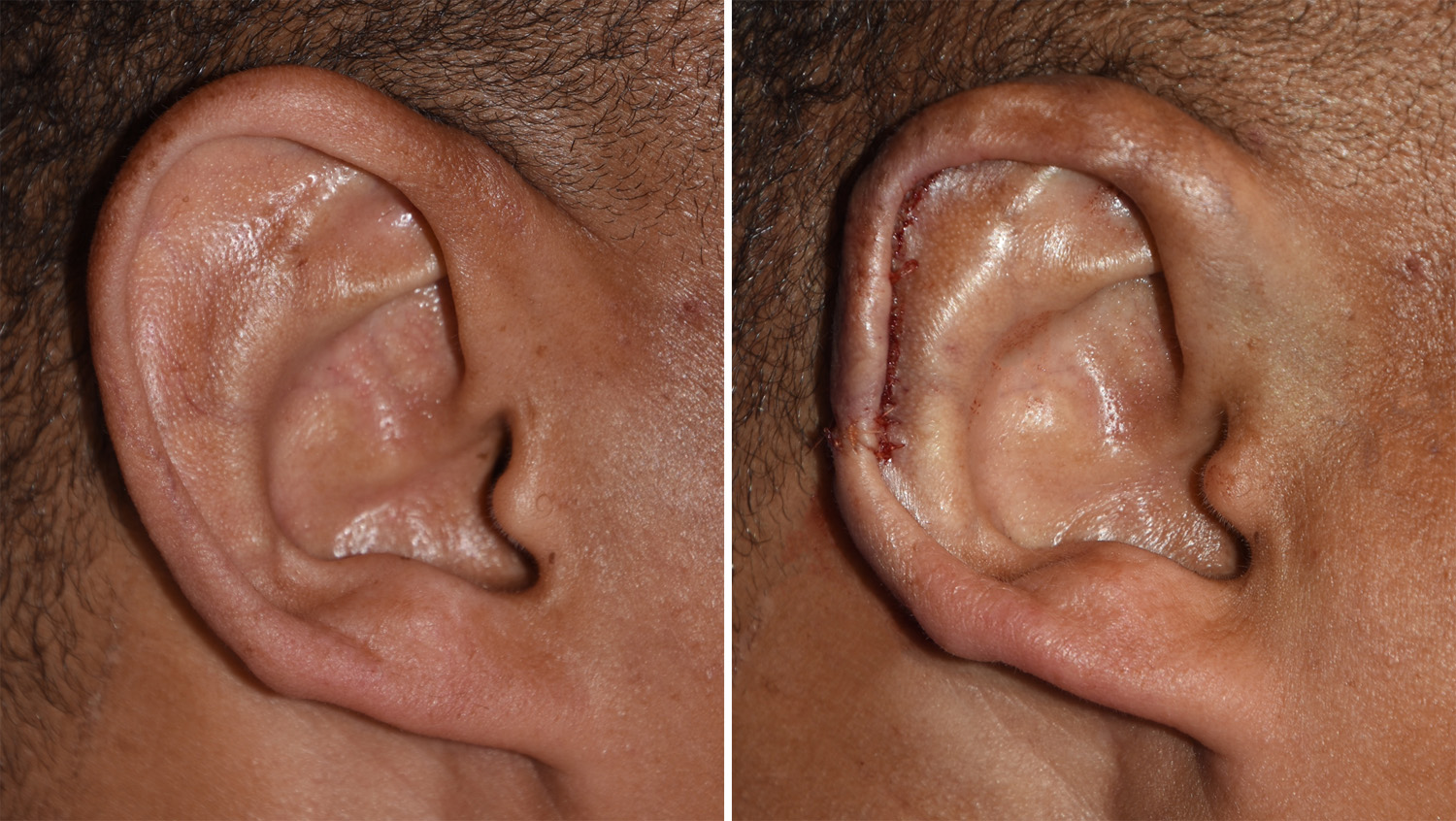
 Under local anesthesia and IV sedation, a macrotia reduction procedure was done. It was limited to just an upper ear reduction due to the small size of his earlobes. A scaphal flap technique was with a horizontal excision across the helical rim at its middle outer portion. A 7mm reduction of skin and cartilage was done. Vertical ear height measurements at the end of the procedure was 65mms.
Under local anesthesia and IV sedation, a macrotia reduction procedure was done. It was limited to just an upper ear reduction due to the small size of his earlobes. A scaphal flap technique was with a horizontal excision across the helical rim at its middle outer portion. A 7mm reduction of skin and cartilage was done. Vertical ear height measurements at the end of the procedure was 65mms.
The scaphal flap technique in macrotia reduction is an cartilage-skin flap that remains viable due to the attachment of the postauricular skin. When the outer ear height is shortened and closed, this creates ‘dogears’ on the back of the ear. These are removed as the final step in the procedure by removal of redundant skin folds in a vertical pattern that lies parallel to the helical rim.
Highlights:
1) Reduction of large ears us usually done by reducing the top and the bottom of the ear.
2) With a normal sized earlobe, macrotia reduction must be done by an upper helical scaphal flap reduction method.
3) Macrotia reduction is done under local anesthesia in most patients.
Dr. Barry Eppley
Indianapolis, Indiana