

Background: The ear has a complex structure that is often unappreciated due to its relative obscurity on the side of the head. But when something about its structure makes it stand out, it becomes open to considerable aesthetic scrutiny. The most common aesthetic distractor is when the ear sticks out too far from the side of the head or when it has congenital deficiencies in its structure.
One very noticeable aesthetic deformity of the ear its when it is too large or vertically long. While there are numbers for normal ear sizes and relationships to other structures of the face (e.g., nose), what ultimately matters is whether the patient thinks that it is too large. Usually patients are quick to notice earlobes that are too long or hang too low. But large conchal bowls or upper ears can also be points of aesthetic concern.
Ear reduction or macrotia surgery is much more rarely performed than of the protruding ear which can also be called large ear reduction. (even though the actual ear is not too large and no parts of the ear is being resected) Macrotia reduction surgery must remove actual portions of ear structure (skin and cartilage) to create a visible reduction in the size of the ear but also must do with the location of the scars in mind so as to not create an aesthetic distraction.
Case Study: This 35 year-old male had been bothered by the size of his ears since he was young. He had undergone a setback otoplasty and wedge earlobe reduction but this did not make his ears look any smaller. He had a vertically long earlobe and a wide scapha between the helical rim and the superior crus in the upper third of his ear. His vertical ear length was 72mms
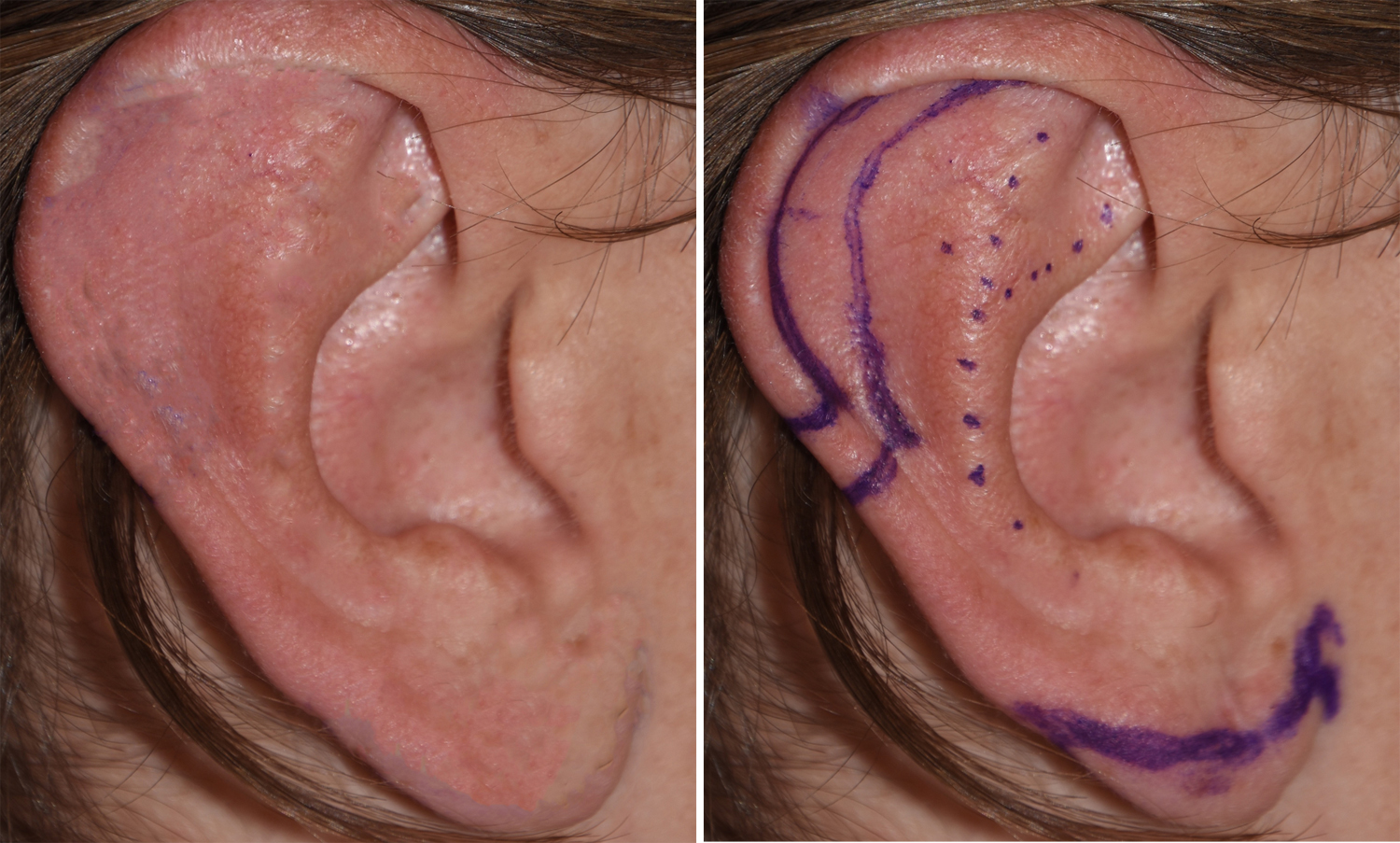
 His macrotia reduction plan was to reduce the upper size of the ear through a scaphal flap with 5mm mid-helical rim reduction. The earlobe would be vertically reduced through an inferior rim resection technique of 7mms.
His macrotia reduction plan was to reduce the upper size of the ear through a scaphal flap with 5mm mid-helical rim reduction. The earlobe would be vertically reduced through an inferior rim resection technique of 7mms.

 Under local anesthesia using a periauricular regional bloc technique, the scaphal flap and earlobe reductions were completed using all dissolvable sutures. His immediate post results show an ear reduction with the vertical length reduced to 64mms.
Under local anesthesia using a periauricular regional bloc technique, the scaphal flap and earlobe reductions were completed using all dissolvable sutures. His immediate post results show an ear reduction with the vertical length reduced to 64mms.
Macrotia reduction requires the removal of ear tissues and the creation of scars. With the scaphal flap and inferior rim earlobe reduction techniques, the only scar of any consequence is the one that crosses the helical rim in the middle of the ear. This small scar usually heals extremely well and has yet to be one that any patient had asked me to revise.
Highlights:
- Macrotia reduction often involves a ‘high and low’ approach to be most effective.
- Scaphal reduction of the upper ear and vertical reduction of the earlobe are the two principal elements of macrotia reduction.
- Reduction of the large ear can be done under local anesthesia using periauricular ring blocks.
Dr. Barry Eppley
Indianapolis, Indiana