

Background: While men have greater brow bone prominences than women, there are cases where the brow bones do overgrow. When they do so the brow bone appear too prominent (Neanderthal-like), the forehead appears retroclined and one’s appearance is harsh or angry looking. While there are different degrees of brow bone hypertrophy in men, ultimately all that matters from a surgical standpoint is whether the individual thinks they are too big.
All male brow bone reductions in my experience require a bone flap setback technique and not just bone burring. The bone over the frontal sinus is not thick enough to allow for more than a few millimeters of retrusion. Removing the bone over the frontal sinus allows for a more significant reduction through the combination of perimeter burring reduction as well as bone flap thinning and reshaping.
In the bone flap brow bone reduction method, ensuring adequate bony coverage of the frontal sinus is important. While no bone flap method ever achieves an air tight seal when replaced, and some small bone defects around the perimeter are always tolerated and go on to heal, larger defects should they occur must be reconstructed.
Case Study: This young male was bothered by his large brow bone protrusion. He reported a history of it growing in the last few years as it did not look protrusive when he was younger. While he had a mildly retroclined forehead above the brow bones, their prominence magnified that effect.
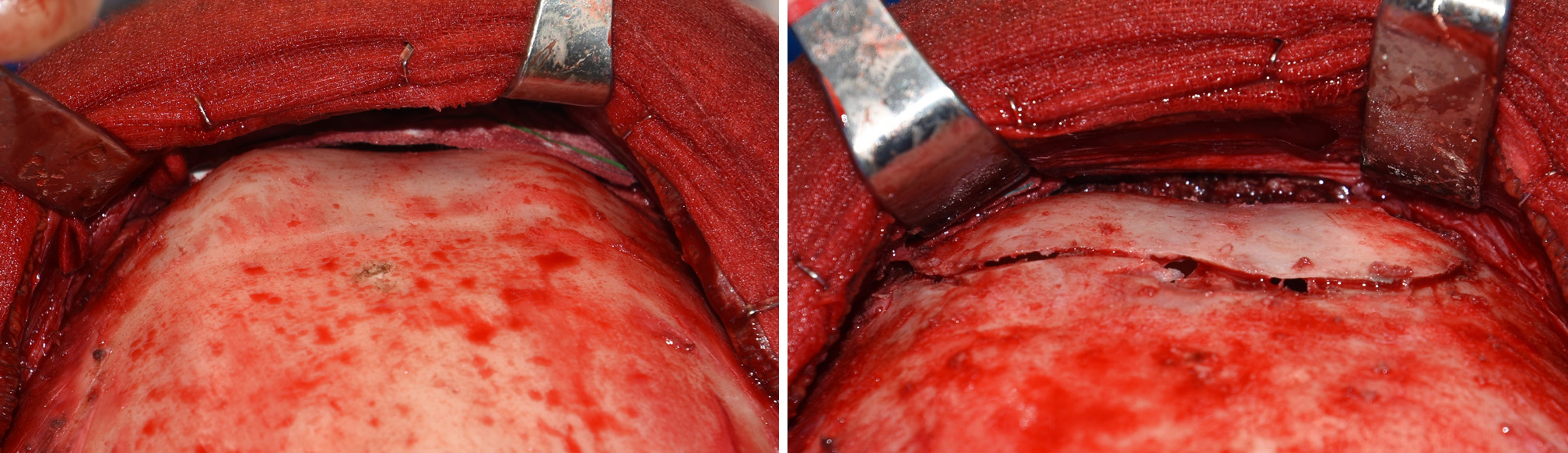
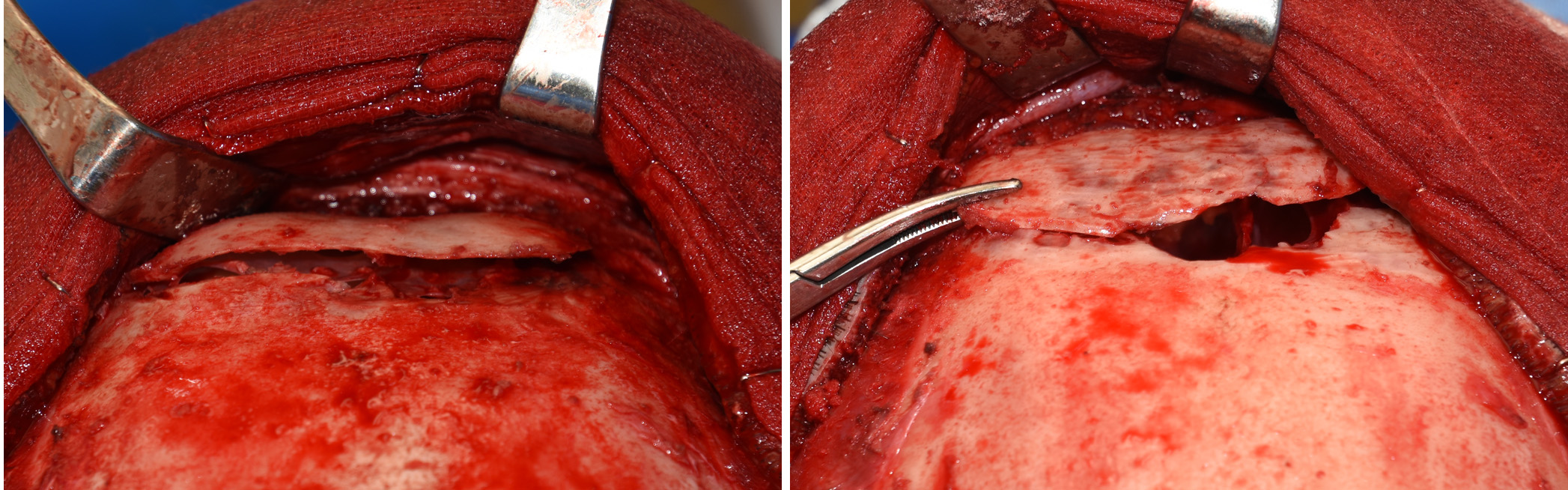 Under general anesthesia and through a near complete coronal scalp incision, the forehead and brow bones were exposed. A reciprocating saw and osteotomes were used to remove the bone over the frontal sinuses. The bone around the flu removal was burred down as well as along the lower brow bones. The bone flap was thinned out and straightened. When putting back the bone flap it could be seen that the front sinus defect was bigger than that of the bone flap…a defect too large to just leave uncovered.
Under general anesthesia and through a near complete coronal scalp incision, the forehead and brow bones were exposed. A reciprocating saw and osteotomes were used to remove the bone over the frontal sinuses. The bone around the flu removal was burred down as well as along the lower brow bones. The bone flap was thinned out and straightened. When putting back the bone flap it could be seen that the front sinus defect was bigger than that of the bone flap…a defect too large to just leave uncovered.
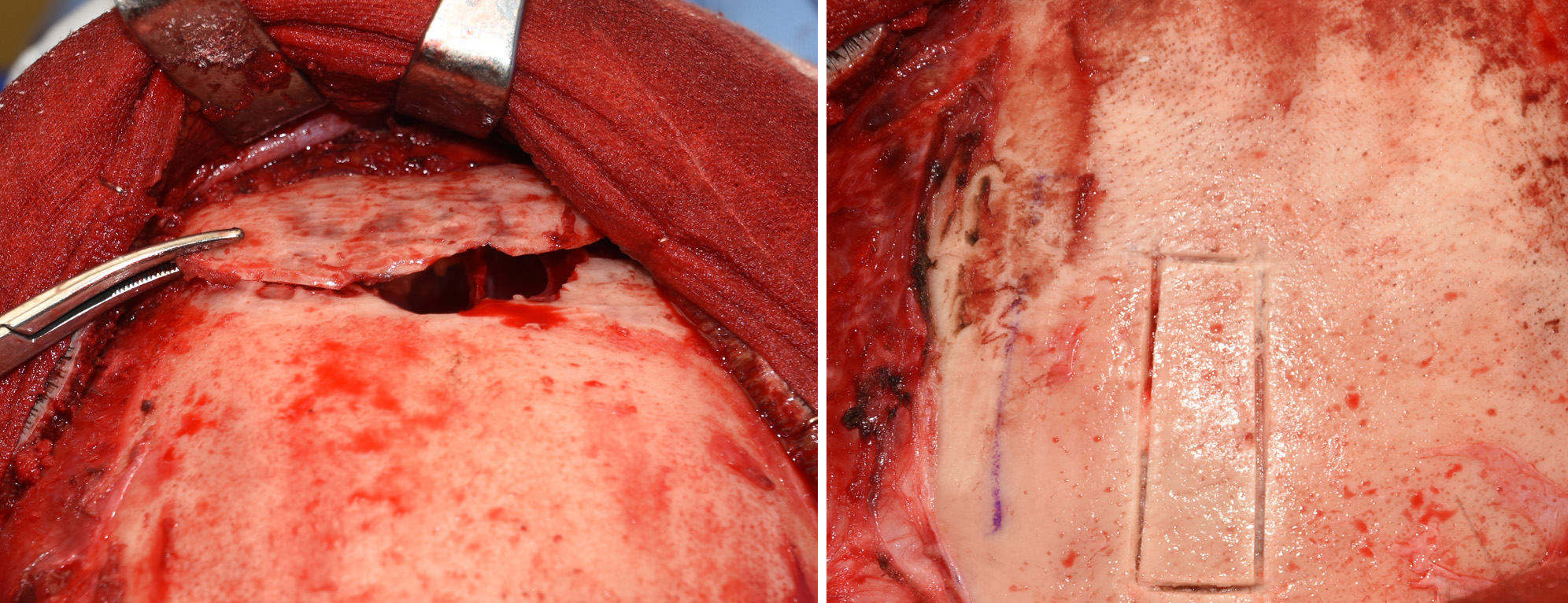
 A 1 x 4 cm split-thickness cranial bone graft was harvested and used to create the additional bone needed to provide a more complete frontal sinus cover.
A 1 x 4 cm split-thickness cranial bone graft was harvested and used to create the additional bone needed to provide a more complete frontal sinus cover.
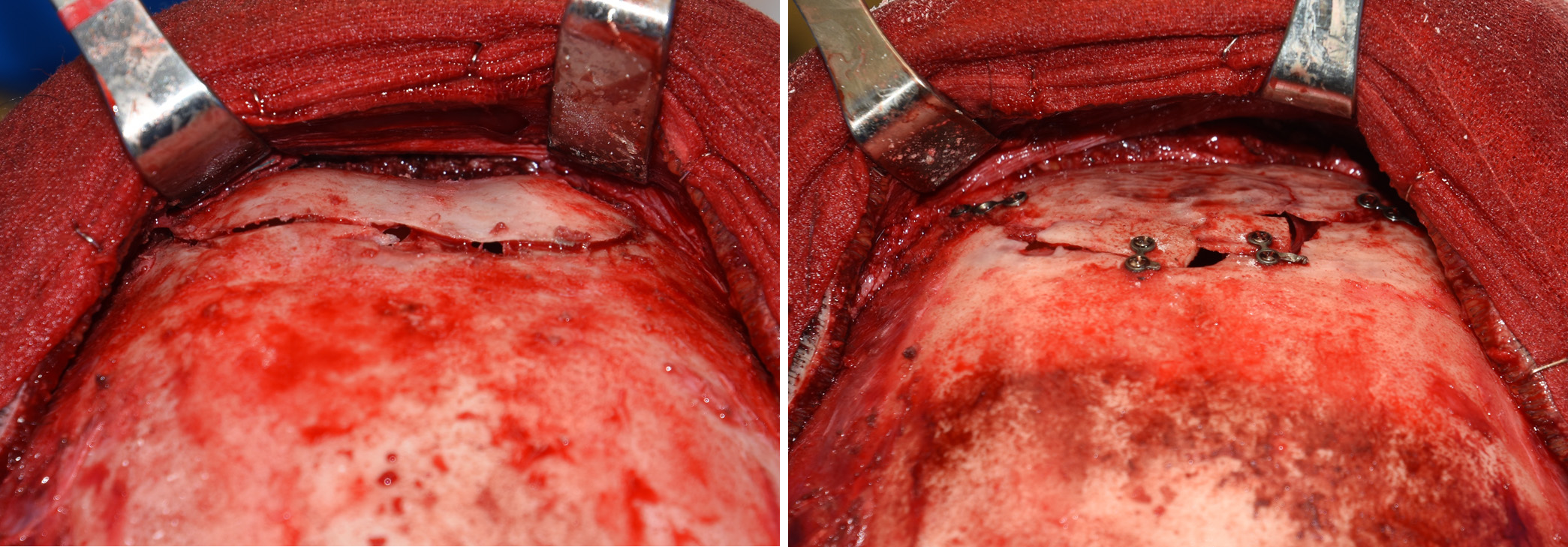
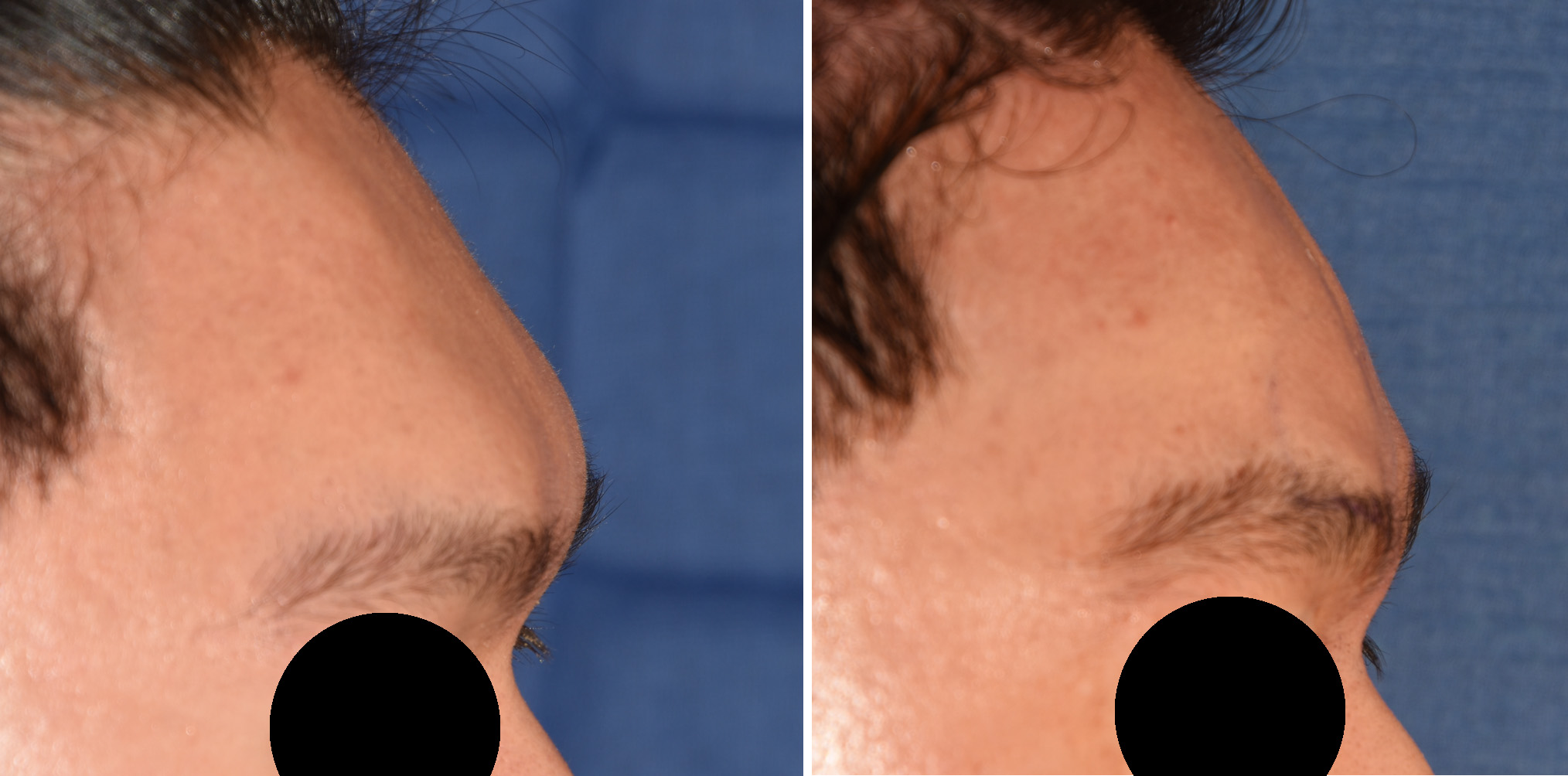 His immediate intraoeprative result showed the reduction in the amount of brow bone protrusion without feminizing his forehead appearance.
His immediate intraoeprative result showed the reduction in the amount of brow bone protrusion without feminizing his forehead appearance.
Case Highlights:
1) Significant brow bone reduction requires a bone flap removal, reshaping and replacement approach.
2) Brow bone flaps require burring of both the surrounding bone prior to replacement as well as thinning of the bone flap itself.
3) In rare cases a cranial bone graft may be needed to fill in any large bone defects of the frontal sinus.
Dr. Barry Eppley
Indianapolis, Indiana