

Background: Rhinoplasty surgery can create many changes to the shape of the nose from its union with the forehead up top down to the base of the nasal tip. One of the top three requested nasal changes is that of a hump or bump. A prominent nasal hump not only distracts from a pleasing nasal shape but it also draws attention away from one’s eyes. The nose should blend into the center of the face and allow the eyes to become a major focal point in both conversation and pictures.
While everyone recognizes a nasal hump, there are misconceptions about what causes it. Most perceive that it is a completely bony structure but a hump is actually where the nasal bones and septal cartilage meet along the bridge of the nose. Its prominence is a function of genetics, ethnicity and how much the underlying septum has grown. Septal overgrowth from below will push up the nasal bones and create an uprising along the dorsal line. In essence, most nasal humps can be seen as half bone (top half) and half cartilage. (bottom half)
Hump reduction involves bone and cartilage removal and is often the first thing done in many rhinoplasty surgeries. While there are differing contributions of bone and cartilage makeup of the nasal hump, both components of it must be taken down to make the hump smaller or disappear. In men the hump must only be reduced enough to have a straight dorsal line propfile. (women can tolerate more of a reduction or lower dorsal line) In some patients, there is a desire to keep a small hump to preserve their ethnicity.
Case Study: This 30 year old hispanic male wanted to get rid of the large hump on his nose. He also wanted the tip of his nose to not droop down so much and to be a little bit thinner. He had some mild breathing difficulties but none that could be attributed specifically to either side of his nose consistently.
 Under general anesthesia, an open rhinoplasty approach was done. The upper lateral cartilages were separated from the top of the septum and the cartilage part of the dorsal line trimmed down. This exposed the end of the nasal bones which were reduced by an osteotome and rasping. The upper lateral cartilages were sewn back to the septum by folding them over onto themselves, creating a form of a spreader graft on each side. The caudal end of the septum and the lower alar cartilages reshaped and sutured together. Low lateral nasal bone osteotomies were done from an intranasal approach.
Under general anesthesia, an open rhinoplasty approach was done. The upper lateral cartilages were separated from the top of the septum and the cartilage part of the dorsal line trimmed down. This exposed the end of the nasal bones which were reduced by an osteotome and rasping. The upper lateral cartilages were sewn back to the septum by folding them over onto themselves, creating a form of a spreader graft on each side. The caudal end of the septum and the lower alar cartilages reshaped and sutured together. Low lateral nasal bone osteotomies were done from an intranasal approach.
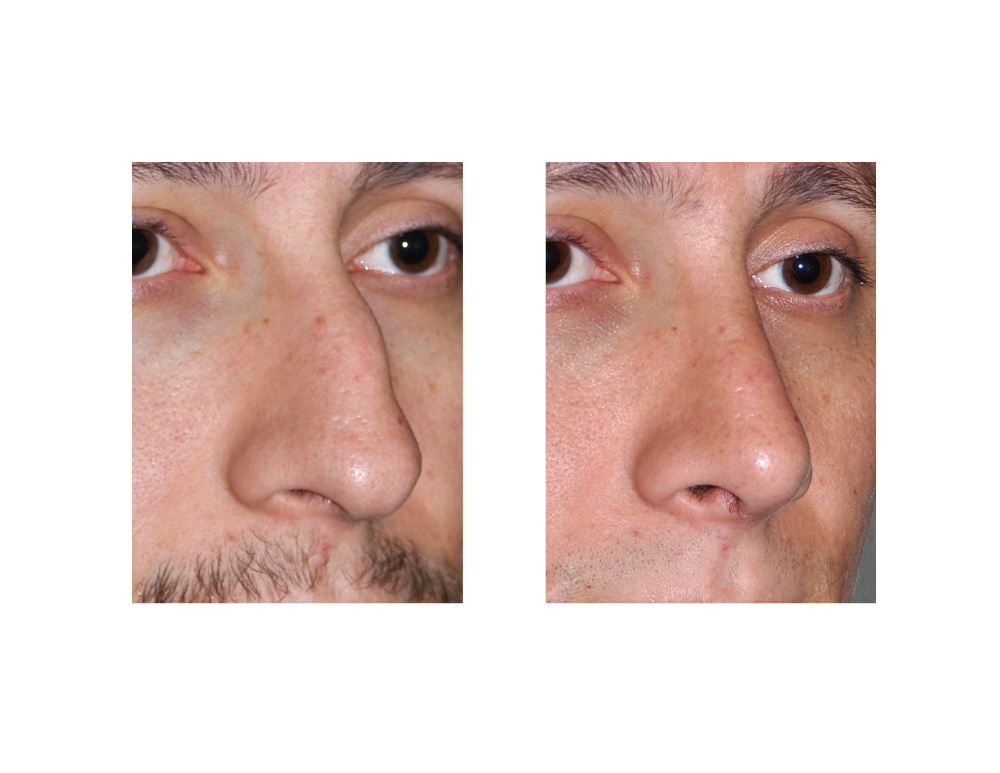 At six weeks after surgery, enough swelling had gone down to reveal a much improved nasal shape. Further nasal tip changes could be expected to occur as further swelling and skin adaptation occurred over the cartilages in the ensuing months.
At six weeks after surgery, enough swelling had gone down to reveal a much improved nasal shape. Further nasal tip changes could be expected to occur as further swelling and skin adaptation occurred over the cartilages in the ensuing months.
Male nasal hump reduction rhinoplasty must take into account how much to reduce its prominence and to prevent middle nasal vault collapse. Smoothness and prevention of over reduction of the bridge are keys in male rhinoplasty. But an overlooked component of dorsal line reduction is in the supratip area. This is the hardest are to judge how much reduction should be done and is frequently overlooked or under reduced in hump reduction. If inadequately reduced a polly beak deformity can result from a residual excess of cartilage height at the lower end of the septal height.
Case Highlights:
1) A nasal hump or bump is one of the most commonly requested reasons for rhinoplasty surgery.
2) Taking down a nasal hump involves both cartilage and bone reduction which may require nasal osteotomies if a residual open roof deformity results.
3) In men, rhinoplasty for hump reduction should strive to attain a string straight dorsal line and avoid over rotation of the nasal tip.
Dr. Barry Eppley
Indianapolis, Indiana