

Background: Gynecomastia, the development of breasts in men, is often thought of as a young man’s problem. While hormonal changes certainly set the stage for the emergence of breasts in some teenagers and young men, similar problems of a slightly different nature occur at the opposite end of the age spectrum.
When older men develop what used to be called ‘senile gynecomastia’ due to testosterone decline, it is not the ‘plump’ type of gynecomastia seen in youth. Rather it is a sagging mass of chest tissue in which the nipple and breast mound sags over the inframammary fold. There is a loss of skin elasticity and ligamentous laxity that allows the chest to fall off of the pectoralis muscle inferiorly.
While liposuction is a frequent treatment for gynecomastia reduction, it will not produce the desired result in many older gynecomastias. While some chest volume reduction will be achieved, the skin will not tighten up and the nipple will not be elevated higher on the chest wall afterwards. Some type of skin excisional chest wall tightening is needed.
When a breast lift is needed, men must be treated differently than women. Men can not have the same type of breast reduction scars since there is no mound to hide them when the lift is completed. It is the vertical scar between the nipple and the fold that would be objectionable in men.
Case Study: This 76 year-old man was bothered by the sagging shape of his chest. He did not like his appearance in shirts and felt he needed a ‘mansier’ to really hold his chest up. While he had some excessive breast tissue, his excessive skin was as much if not more of a problem.
 Prior to surgery, his existing inframammary fold was marked as well as around his areolas. An elliptical excision pattern was then marked from one end of the inframammary fold to the other going above the nipple. Under general anesthesia, a tumescent solution was infiltrated into each side of the chest. Using power-assisted liposuction, 200cc of fat and breast tissue was aspirated from each side. The upper and lower ends of the horizontal excision pattern was incised as well as around the areolas. The intervening skin was de-epithelized. An upper chest skin flap was raised up near the collar bones on each side. The thinned out breast mound and nipple was then lifted as the skin edge of the raised chest flap was brought down over it. The new position of the nipples were marked and the overlying skin removed. The nipples were brought through and the circumareolar and inframammary skin edges were then closed to complete the reduction. The nipple transposition eliminated any need for a vertical scar.
Prior to surgery, his existing inframammary fold was marked as well as around his areolas. An elliptical excision pattern was then marked from one end of the inframammary fold to the other going above the nipple. Under general anesthesia, a tumescent solution was infiltrated into each side of the chest. Using power-assisted liposuction, 200cc of fat and breast tissue was aspirated from each side. The upper and lower ends of the horizontal excision pattern was incised as well as around the areolas. The intervening skin was de-epithelized. An upper chest skin flap was raised up near the collar bones on each side. The thinned out breast mound and nipple was then lifted as the skin edge of the raised chest flap was brought down over it. The new position of the nipples were marked and the overlying skin removed. The nipples were brought through and the circumareolar and inframammary skin edges were then closed to complete the reduction. The nipple transposition eliminated any need for a vertical scar.

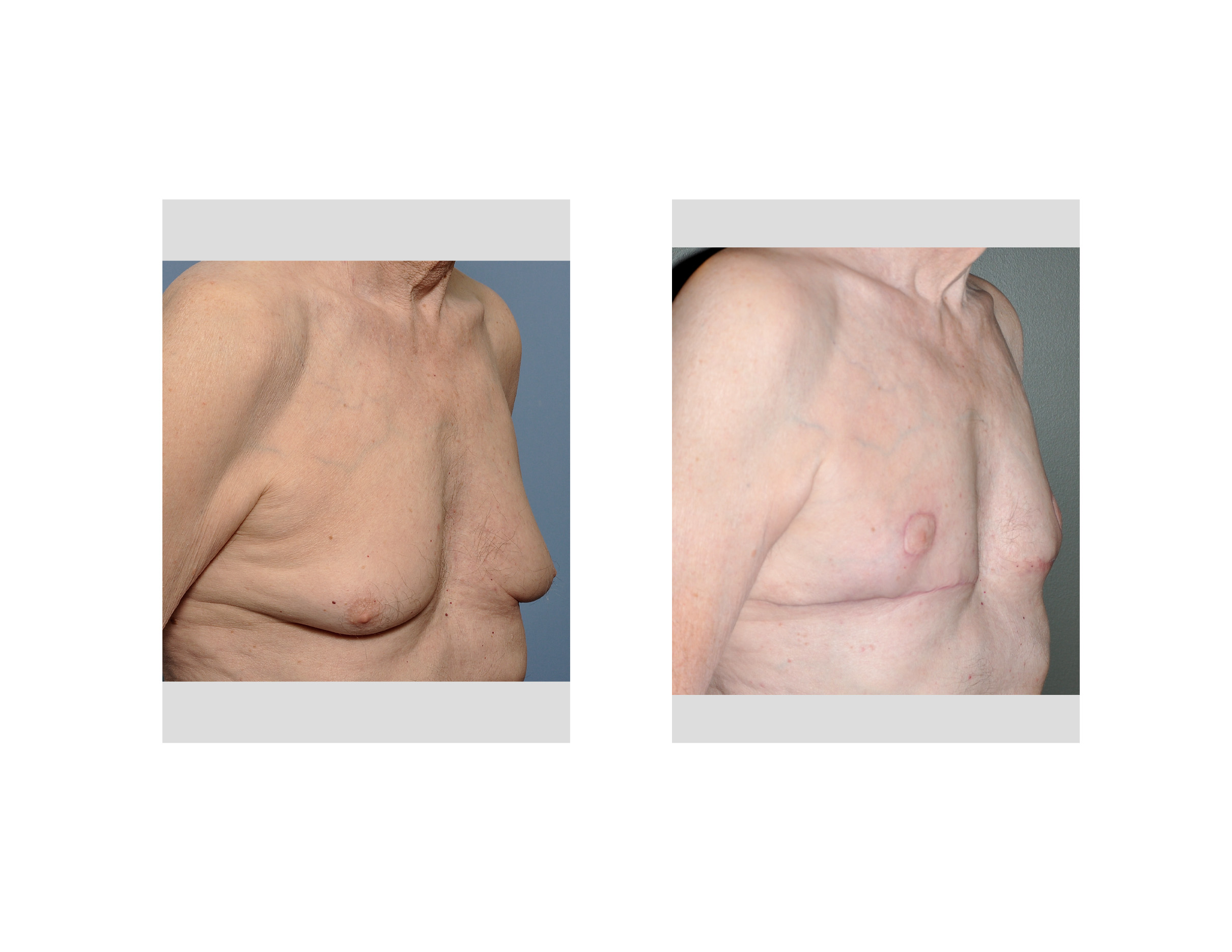 He had drains that were removed two days later and the incisions remained taped for ten days as he wore a circumferential chest compression wrap. When seen at six weeks after surgery, his chest was flat and the nipples in a much more uplifted position. It would take another 3 to 6 months for the scars to completely mature and fade.
He had drains that were removed two days later and the incisions remained taped for ten days as he wore a circumferential chest compression wrap. When seen at six weeks after surgery, his chest was flat and the nipples in a much more uplifted position. It would take another 3 to 6 months for the scars to completely mature and fade.
 For the man who has significant chest sagging and requires a breast lift, gynecomastia reduction with nipple transposition creates an acceptable location of the scars.
For the man who has significant chest sagging and requires a breast lift, gynecomastia reduction with nipple transposition creates an acceptable location of the scars.
Case Highlights:
1) The older male patient often develops chest sagging that is difficult to hide and not cured by exercise.
2) With loose and inelastic skin due to age, liposuction does not produce a satisfactory gynecomastia reduction for many older men.
3) Gynecomastia reduction with nipple transposition is the most effective chest reshaping method for the older male with ‘man boobs’.
Dr. Barry Eppley
Indianapolis, Indiana