

Background: The formation of the ear is an amazingly complex embryonic process. That is evident in just looking at the ear with its spiral array of convexities and concavities of cartilage around the ear canal. It is remarkable that it forms properly and does so twice in most people due to its bilateral presence.
But because of its complexity the ear is one of the most commonly misshapen of all facial features. From minor deformities like earlobe clefts and Stahl’s ear to major malformations like microtia there is a wide array of congenital ear malformations that can occur. One of the most common ear anomalies, and it is questionable whether it should be called an anomaly, is that of the protruding ear. All of the ear is present but its sticks out too far from the side of head due to the lack of an antihelical fold, overgrowth of the concha or some combination of both.
Setback otoplasty, also called ear pinning, is the well recognized surgery for the correction of the excessively protruding ear. It is done in both adults and children. The common question in children is at what age is the proper time to perform the surgery. The underlying premise of this question is when can the surgery be done so that it will not adversely affect growth of the ear cartilage.
Case Study: This 6 year-old male child has very prominent ears due primarily to a lack of antihelical fold development. Where the fold was completely absent the ear stuck out the most. Down near the earlobe some sembence of an antihelical fold was present and the ear stuck out less.
 Under general anesthesia an otoplasty procedure was performed through an incision on the back of his ears. Minimal skin was removed from the back of the ear and the correction was done principally through multiple horizontal mattress sutures (to create the fold) and some concha-mastoid sutures. (to decrease the auriculo-cephalic angle)
Under general anesthesia an otoplasty procedure was performed through an incision on the back of his ears. Minimal skin was removed from the back of the ear and the correction was done principally through multiple horizontal mattress sutures (to create the fold) and some concha-mastoid sutures. (to decrease the auriculo-cephalic angle)

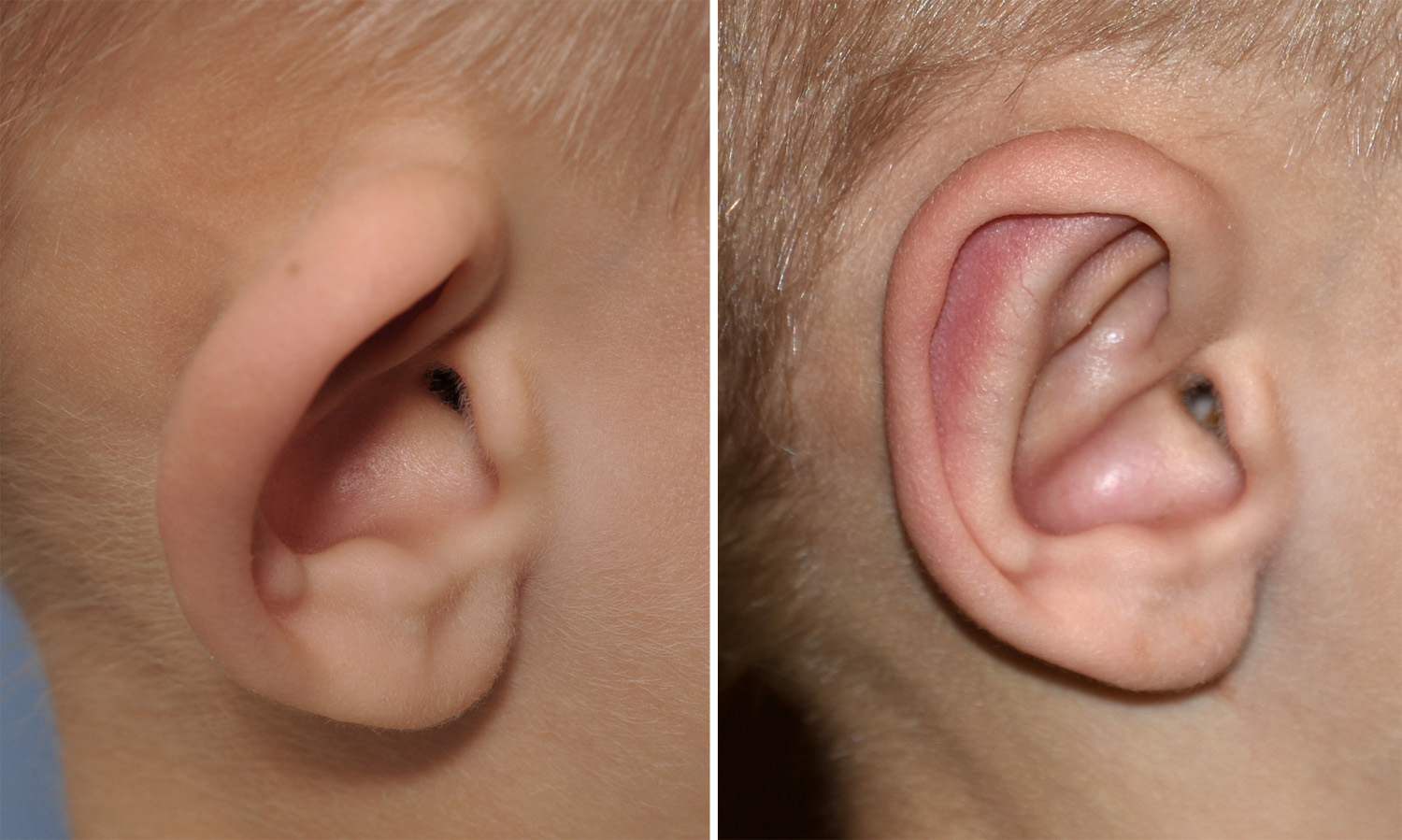 His one month results show a good and reasonable symmetric ear reshaping result. A close-up side view of before and after pictures show that the effect was largely achieved by creating an antihelical fold and a more defined superior crus in the upper helix.
His one month results show a good and reasonable symmetric ear reshaping result. A close-up side view of before and after pictures show that the effect was largely achieved by creating an antihelical fold and a more defined superior crus in the upper helix.
Clinical studies have shown that suture cartilage manipulation of the ear can be done as early as age 2 without any negative growth effects on the ear cartilage. While it can be technically done at such as early age (and I have done so numerous times) there is the important question of postoperative compliance and avoidance of unintentional ear trauma. (which could cause suture disruption and partial ear shape relapse) Between lack of any psychosocial developmental issues in children and performing elective surgery at such a young age, it is far more common to have pediatric otoplasty done closer to age 5 or 6.
Highlights:
1) Congenital ear deformities are amongst the most frequently occurring of all facial deformities of which the protuding ear is the most common one seen.
2) Setback otoplasty (ear pinning) achieves its effect primarily by cartilage bending.
3) The age to perform an otoplasty is largely parent driven in children and be effectively done anytime after age 2.
Dr. Barry Eppley
Indianapolis, Indiana