

Background: Otoplasty is the most form of ear reshaping surgery. Even though the term otoplasty is a general one it is typically associated with treating the protruding ear. The ear that sticks out is due to excessive conchal cartilage, lack of an adequate antihelical fold or both. Changing this undesired ear shape is done by bending or folding the cartilages and then holding them into the new shape with permanent sutures.
The result from such otoplasty cartilage reshaping maneuvers has a large intraoperative artistic component. How much the cartilage is folded and setback, how many sutures to place and judging the new look are all up to the discretion of the surgeon. The outcome is made doubly challenging because there are two ears and going back and forth between them to achieve the best symmetry requires a lot of artistic judgment.
There is always the risk needing a revision from otoplasty surgery due to asymmetry or an undesired ear shape. An underdone otoplasty outcome can be satisfactorily treated by increasing the amount of the cartilage fold by placing new sutures. Correcting an overdone otoplasty, however, is not as simple as just releasing the old sutures or placing new ones. A different approach is needed to partially reverse an ear cartilage fold.
Case Study: This 6 year-old male child had an ‘incisionless otoplasty’ one year previously. The right ear shape outcome was satisfactory but the left ear looked completely different. The conchal aspect of the left ear was too protrusive and the upper ear antihelical fold was turned back too far.
 Under general anesthesia the back of the left ear was opened and the cartilages exposed. A small conchal cartilage graft was harvested and the concha set back by concha-mastoid sutures. The antihelical fold sutures were released but that did not change its shape. An interpositional conchal cartilage graft was placed to help hold out the antihelical fold into a better ear shape. This combination of ear reshaping maneuvers achieved bette symmetry to the opposite ear.
Under general anesthesia the back of the left ear was opened and the cartilages exposed. A small conchal cartilage graft was harvested and the concha set back by concha-mastoid sutures. The antihelical fold sutures were released but that did not change its shape. An interpositional conchal cartilage graft was placed to help hold out the antihelical fold into a better ear shape. This combination of ear reshaping maneuvers achieved bette symmetry to the opposite ear.
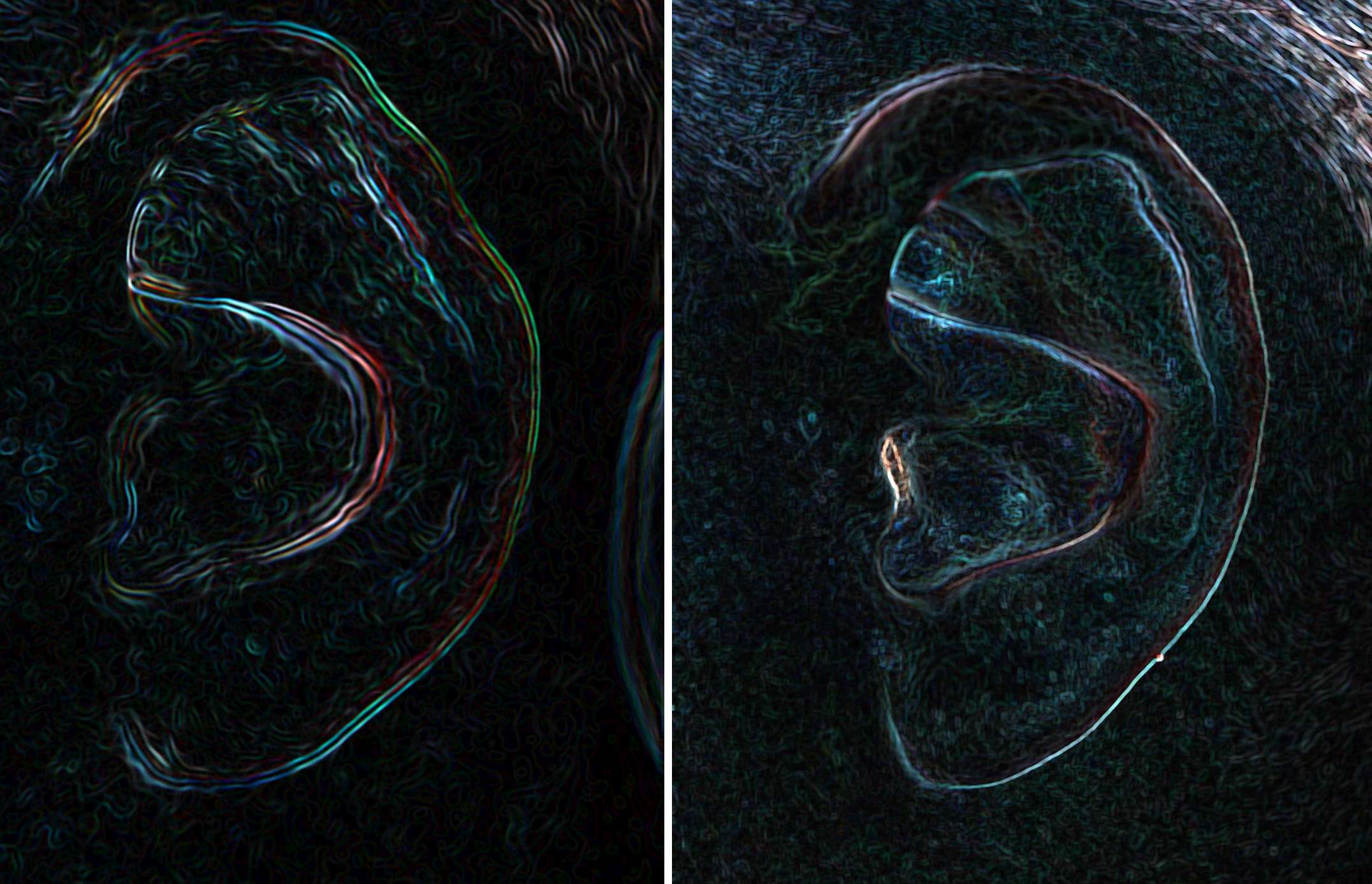 The difference in the cartilage shape of the ear can be seen in this edge highlighting method.
The difference in the cartilage shape of the ear can be seen in this edge highlighting method.
A reversal otoplasty is rarely as simple as just releasing sutures or the scar tissues between the cartilage fold. Memory of the cartilage does persist for some time and probably does so in children longer than in adults. But once a year after surgery has passed the memory of the original cartilage shape has been lost. To hold out or to partially reverse an antihelical fold an interpositional spacer graft is needed. Autologous cartilage is always the best spacer graft for a reversal otoplasty. If it is just one ear it may be possible to harvest the cartilage from the conchal area of the same ear.
Highlights:
1) Ear reshaping from an otoplasty is usually done by folding of the protruding cartilage into a new shape with suture fixation at multiple points.
2) An otoplasty can be overdone when the amount of cartilage folding is excessive and the desired three-tiered structure of the ear is disrupted.
3) A reversal otoplasty is rarely effective done by suture release after the ear is completely healed.
Dr. Barry Eppley
Indianapolis, Indiana