

Background: The amount of protrusion of the ear from the side of the head varies amongst different people. But regardless of the exact auriculocephalic angle an individual has, the frontal view of the ear should show a three-level tier shape. This means there is the concha at the lowest or inner level, the antihelical fold at the middle level and the helical rim is the third or outer level. Like a set of bleacher seats the ear should have these three distinct levels.
Besides congenial deformities this normal shape of the ear can be disrupted by traumatic injuries or surgery. One of the most common causes of affecting the levels of the ear is aesthetic otoplasty surgery. In setting back of the protruding ear, due to lack of an antihelical fold or a large concha, the outer level of the ear (helix) can be pulled back too far. This is known as an over corrected otoplasty and is not rare to occur given that the margin of error in ear reshaping is a matter of milimeters.
Correction of an overcorrected otoplasty, known as a reverse otoplasty or otoplasty reversal, can be done by suture release if done soon after the initial surgery. But once scar tissue has formed and the ear cartilage has lost memory, scar/suture release alone is not enough, it will need to be combined with an interpositional or strut graft to hold the ear back out as it heals.
Case Study: This young male had a history of a cholesteotoma surgery followed by ear canal reconstruction with a conchal cartilage graft. Whether the cartilage ends of the door site was primarily closed or the amount of cartilage taken caused the ear to collapse, the ear became pulled back. The middle third of the ear lost its projection with the outer helix being retracted behind the antihelical fold. The ear was very tight due to the scar contracture. This caused some obvious asymmetry to the opposite ear.
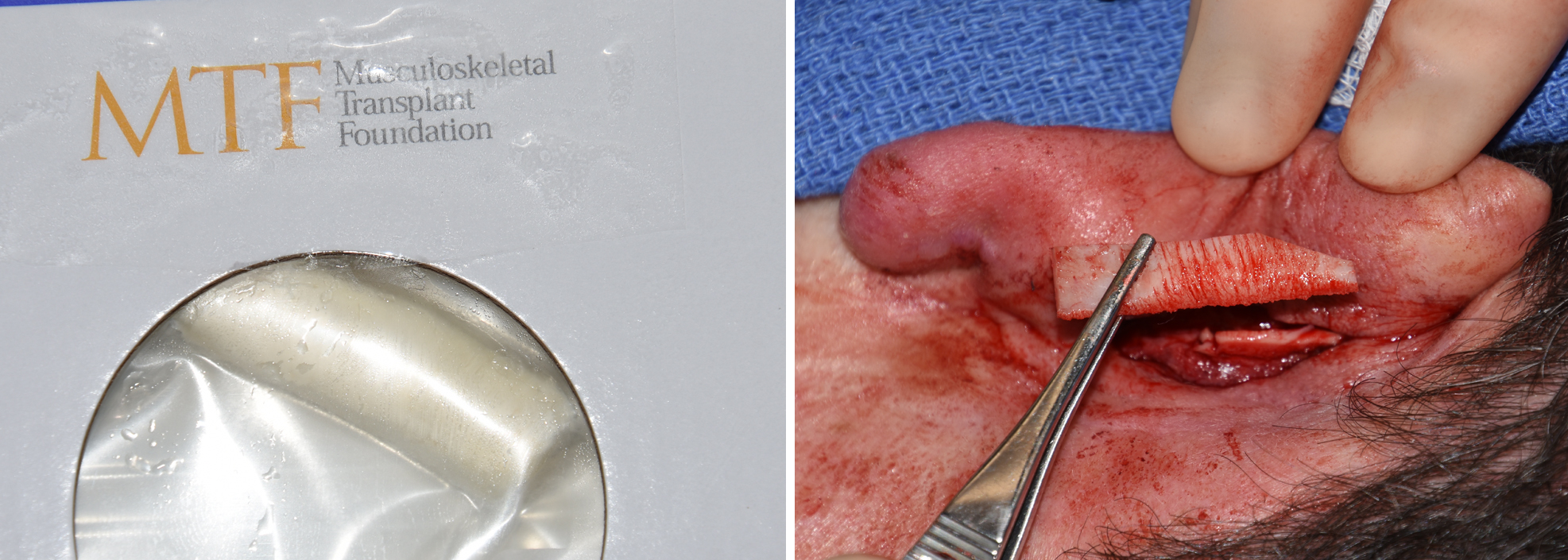
 Under local anesthesia and through the existing postauricular scar, the scarred cartilage ends of the concha were released and the helical rim brought back out. Using cadaveric costal cartilage, two grafts were fashioned and placed as vertical struts between the helical rim superiorly and the mastoid bone inferiorly underneath the postauricular skin. This resulted in firm support of the released outer helical rim of the middle third of the ear.
Under local anesthesia and through the existing postauricular scar, the scarred cartilage ends of the concha were released and the helical rim brought back out. Using cadaveric costal cartilage, two grafts were fashioned and placed as vertical struts between the helical rim superiorly and the mastoid bone inferiorly underneath the postauricular skin. This resulted in firm support of the released outer helical rim of the middle third of the ear.
The fundamental concept of most reverse otoplasties is that support is needed once the cartilage and scar is released. While one’ s own cartilage is always the best graft material, most patients understandably do not want to have a rib graft harvested. Other cartilage harvest sites offer too little material which lacks the rigid support needed. Thus the use of tissue bank or cadaveric rib graft offers a good alternative.
Case Highlights:
1) The natural ear shape has three distinct levels of projection of its cartilaginous parts.
2) Loss of outer hello rim projection creates a pulled back appearance and ear asymmetry.
3) A cadaveric rib graft is a good graft option to support the released ear in a reverse otoplasty.
Dr. Barry Eppley
Indianapolis, Indiana