

Background: Rhinoplasty can create a diverse number of nose shape changes. One of the most commonly requested nose changes, particularly amongst women, is to have more tip rotation. (not hang so low) Overgrowth of the underlying caudal septum and long lower alar cartilages help create the length or amount of projection and rotationof the nasal tip from the rest of the nose. These long tip cartilages almost always cause the nasolabial angle to close down, creating the under rotated tip effect.
In a primary rhinoplasty, the nasal tip can be shortened/lifted through a combination of caudal septal relief and/or lower alar resection through dome or more lateral crural techniques. It is always a challenge to determine how much of these cartilages to remove to provide the amount of tip shortening/rotation desired. And the result from doing these maneuvers is not always prefect particularly in the thick-skinned nose. If the nose is still persistently long or hangs down too low, a revision rhinoplasty may be needed for further tip shortening and/or rotation.
Case Study: This 40 year-old female had two prior rhinoplasties by another surgeon to reshape her nose. This left her with dorsal irregularities and a long and ill-defined tip with inadequate rotation. While she had two prior procedures, she was still interested in trying to make further improvements if possible.
 Under general anesthesia, an open rhinoplasty approach was used. Dorsal smoothing was done by rasping of bone spurs on the upper edges of the nasal bones. The nasal tip was sharply cleaned of all scar tissue over the domes and in the supratip area. A 2mm wedge of cartilage was taken from the upper caudal septum. (septal angle) A dome division technique was used to shorten the tip as well as narrow it and rotate it upward.
Under general anesthesia, an open rhinoplasty approach was used. Dorsal smoothing was done by rasping of bone spurs on the upper edges of the nasal bones. The nasal tip was sharply cleaned of all scar tissue over the domes and in the supratip area. A 2mm wedge of cartilage was taken from the upper caudal septum. (septal angle) A dome division technique was used to shorten the tip as well as narrow it and rotate it upward.

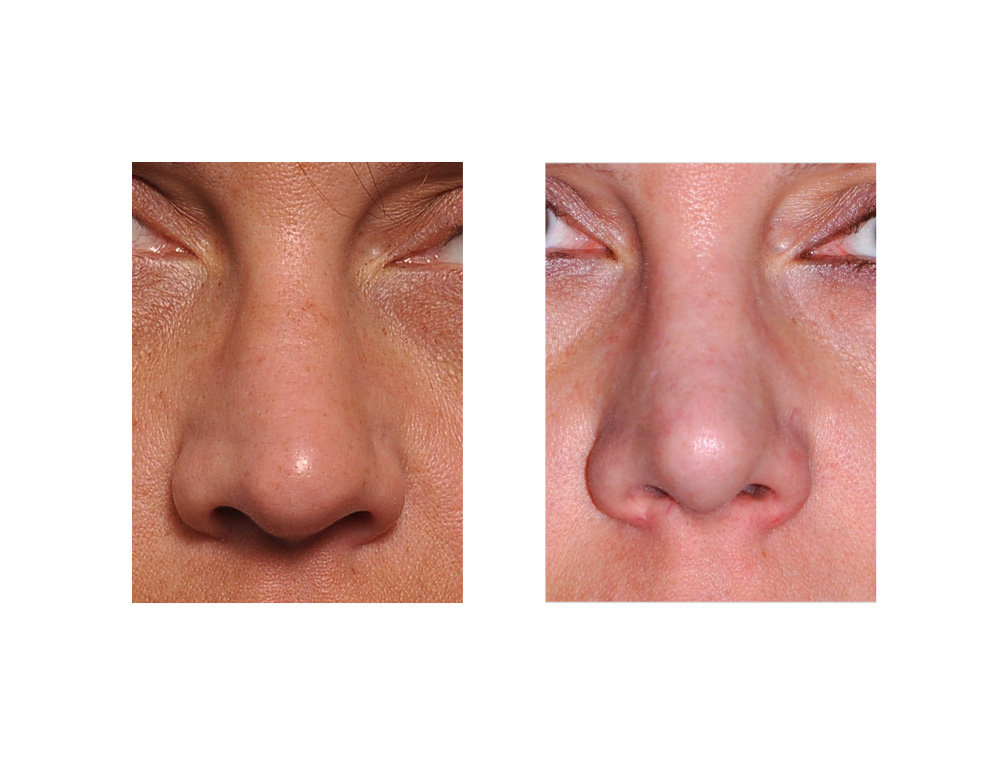 Tertiary rhinoplasty (2nd revision rhinoplasty) has limits as to what can be achieved, particularly in the tip area. Scar tissue and skin changes make it less capable of being shaped and more resistant to efforts at any additional refinement. This is particularly manifest when it comes to giving the thicker skinned nose more rotation and opening up the nasolabial angle. This result demonstrates that changes are possible with visible shortening and rotation but very limited improvement in tip refinement.
Tertiary rhinoplasty (2nd revision rhinoplasty) has limits as to what can be achieved, particularly in the tip area. Scar tissue and skin changes make it less capable of being shaped and more resistant to efforts at any additional refinement. This is particularly manifest when it comes to giving the thicker skinned nose more rotation and opening up the nasolabial angle. This result demonstrates that changes are possible with visible shortening and rotation but very limited improvement in tip refinement.
Case Highlights:
1) Shortening a long nose is a common objective of many rhinoplasty surgeries due to congenital overgrowth of the lower alar cartilages and septum.
2) A long nose can also persist or occur after a primary rhinoplasty from over resection of the dorsum and/or failure to remove adequate cartilage from the nasal tip.
3) Revision rhinoplasty can correct the residual long nose through conventional tip shortening/reshaping techniques but further tip narrowing refinement may be elusive
Dr. Barry Eppley
Indianapolis, Indiana