

Background: While patients born with cleft lip and palate have obvious lip, jaw and palate abnormalities, the nose that sits above it is equally affected. It may not be actually cleft but it suffers a variety of well described asymmetries and deficiencies. Internally, the septum is severely deviated away from the cleft side which results in cleft side inferior turbinate hypertrophy. The external nasal tip is deviated with slumping of the nostril rim on the cleft side, a widened nostril and loss of nasal sill definition. The nasal bridge often looks like a hump but may only appear so because the nasal tip lacks definition and is too low.
While not present is every cleft nose, the nasal skin is often very thick particularly over the nasal tip. Why the cleft nasal skin is often thick is not known but poses its own problem in cleft rhinoplasty surgery. The cleft nose always suffers from some deficiency of tissues over the tip area. The deficiency of skin is along the nostril rim and nasal base on the cleft side in unilateral patients and along both the columella and both nostril rims in bilateral cleft patients.
Getting the tip of the cleft nose built out requires substantial cartilage support in many cases. Good structural support is needed to lift the thick nasal skin out and resist postoperative contracture. While the septum and ears are good sources of cartilage for grafting in rhinoplasty, they may not be enough for a complete cleft septorhinoplasty.
Case Study: This 42 year-old female was originally born with a left unilateral cleft lip and palate deformity. While her lip, alveolus and palate were reasonably well repaired, she remained with a misshapen nose that had limited airflow through it.

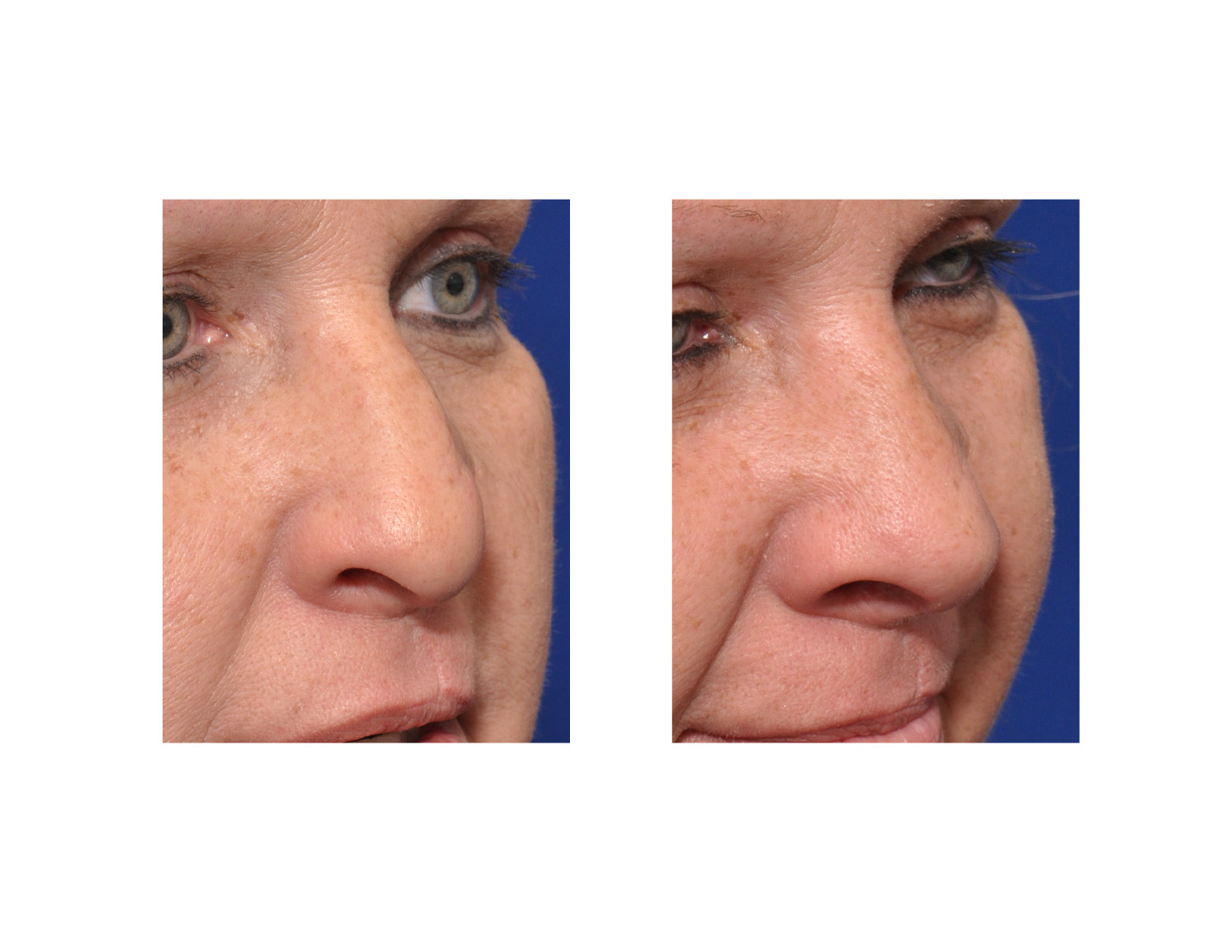 Under general anesthesia, she initially had free floating rib # 9 harvested and a small straight piece of cartilage taken from #8 by an in situ harvest technique. Through an open rhinoplasty, her septum was straightened and excess cartilage removed. The right inferior turbinate underwent subtotal resection while the left inferior turbinate was cauterized and outfractured. The external nose was reshaped and structurally rebuilt using middle vault spreader grafts, a columellar strut, a septal extension graft and bilateral lower alar rim batten grafts, all fashioned from the rib grafts.
Under general anesthesia, she initially had free floating rib # 9 harvested and a small straight piece of cartilage taken from #8 by an in situ harvest technique. Through an open rhinoplasty, her septum was straightened and excess cartilage removed. The right inferior turbinate underwent subtotal resection while the left inferior turbinate was cauterized and outfractured. The external nose was reshaped and structurally rebuilt using middle vault spreader grafts, a columellar strut, a septal extension graft and bilateral lower alar rim batten grafts, all fashioned from the rib grafts.
 When performing a cleft septorhinoplasty in adults, the success of the procedure can be highly influenced by the cartilage graft material used to do it. Deficiency of the amount of cartilage graft material or lack of adequate structural integrity or shape of the cartilage can affect the nasal shape outcome. A rib graft harvest avoids this problem by providing more then enough structural support in the difficult cleft septorhinoplasty patient.
When performing a cleft septorhinoplasty in adults, the success of the procedure can be highly influenced by the cartilage graft material used to do it. Deficiency of the amount of cartilage graft material or lack of adequate structural integrity or shape of the cartilage can affect the nasal shape outcome. A rib graft harvest avoids this problem by providing more then enough structural support in the difficult cleft septorhinoplasty patient.
Highlights:
- The definitive septorhinoplasty procedure in cleft and palate patients awaits the late teens or early adulthood age.
- The need for substantial cartilage grafting to build out the tip of the cleft nose often requires a small rib graft for adequate material.
3) With changes to the external nose, septal straightening straightening, inferior turbinate reduction and reconstruction of the middle vault all help to improve nasal breathing.
Dr. Barry Eppley
Indianapolis, Indiana