

Background: One of the main features of the nose is the dorsal line or the nasal dorsum. It is more commonly called the “bridge” of the nose as it connects the forehead to the tip of the protruding nasal tip. It is made up of bone (upper half or upper third) and cartilage. (upper lateral cartilages) In the profile or side view the nasal dorsum should be a relatively smooth continuous line from the forehead to the tip. When looking at the nose from straight on, the dorsum should form straight appearing lines down its sides (dorsal aesthetic lines) that connect the eyebrows to the tip of the nose.
The most frequently encountered aesthetic deformity of the nasal dorsum is that of a hump. (convexity)A dorsal hump is incredibly common and its reduction is done in many a primary rhinoplasty procedure. It results from an overgrowth of the osteocartilaginous junction of the nose and is thus a natural feature. A dorsal depression or saddle nose (concavity) is more times than not an unnatural feature caused by either trauma or iatrogenic causes. (over reduction of a dorsal hump from a rhinoplasty) But it can occur naturally is smaller more upturned noses and is a result of relative undergrowth of the nasal septum during development.
While the dorsal hump requires osteocartilaginous reduction, the dorsal depression requires augmentation. There are multiple methods of nasal dorsal augmentation from implants to cartilage and bone grafts, each with their own advantages and disadvantages.
Case Study: This 24 year-old male wanted to have the dip in his nasal bridge augmented to the point where it was straight. This was a natural dorsal line concavity which he had always had. He had a prior nasal dorsal augmentation with layered septal cartilage, which provided some modest improvement, but not to the level of it being straight. While he realized a dorsal nasal implant could be used, he preferred the use of his own cartilage.
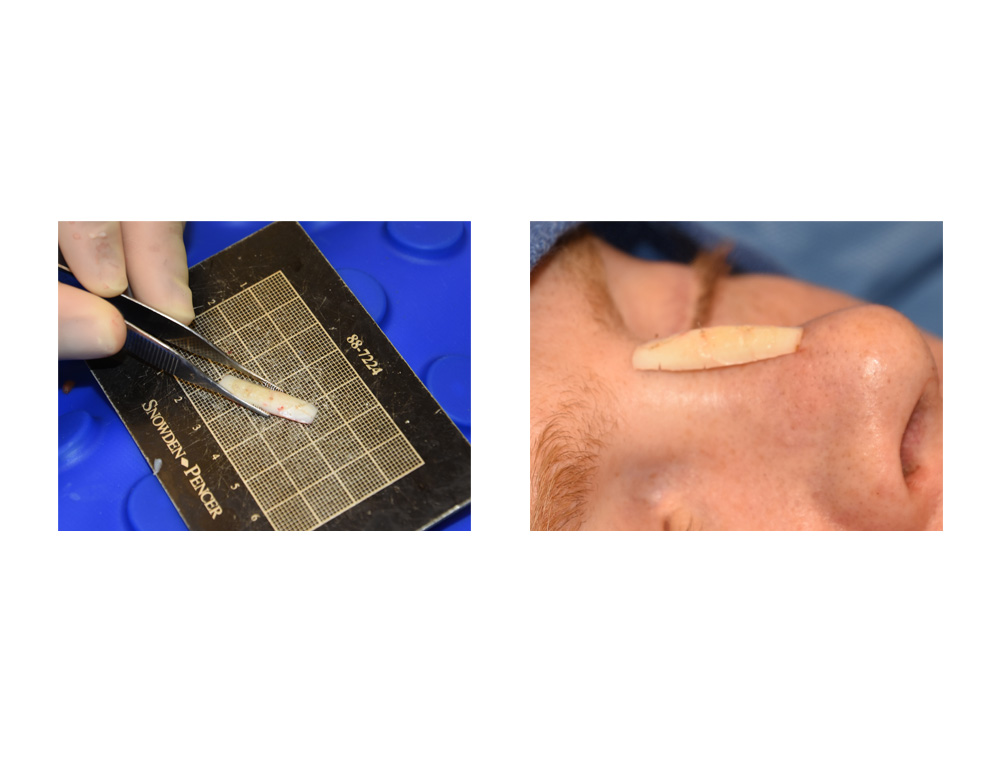
 Under general anesthesia a small rib graft was harvested in situ from the 8th rib through a small 2.5 cm incision. The rib segment was carved to the desired shape and length as measured on the patient’s nose over the area of the depression. Through an intercartilaginous intranasal incision a narrow pocket was developed over the cartilage and bone of the dorsal depression onto which the fashioned cartilage graft was inserted and placed.
Under general anesthesia a small rib graft was harvested in situ from the 8th rib through a small 2.5 cm incision. The rib segment was carved to the desired shape and length as measured on the patient’s nose over the area of the depression. Through an intercartilaginous intranasal incision a narrow pocket was developed over the cartilage and bone of the dorsal depression onto which the fashioned cartilage graft was inserted and placed.
The nasal dorsum can be augmented with a variety of implants and natural tissue grafts. Small nasal dorsal deperssions can be easily and simply built up with implants of various materials. Small silicone dorsal implants are one example and they all offer the assurance of a dorsal augmentation that will not warp later. (although asymmetry can exist if careful pocket development and placement is not done) This small nasal implant also has a very low rate of complications given that it is putting little pressure on the overlying soft tissues.
Despite the simplicity of implants some patients may feel more comfortable with a cartilage graft. While the usual source of harvest is the nasal septum, it is suitable for very limited amounts of dorsal augmentation. Once partially harvested the septum can no longer be considered a donor source. Ear cartilage is curved and the risks of asymmetries and irregularities is high unless it is diced and wrapped in fascia. Small cartilage grafts can be harvested from the rib without having to remove a larger segment by an in situ harvest method.
Highlights:
1) Dorsal augmentation of the nose can be done by either implants or cartilage grafts.
2) A dorsal nasal implant that is modest in size has a very low risk of long-term problems.
3) A single en bloc carved piece of rib can provide a cartilaginous option for dorsal nasal augmentation in rhinoplasty.
Dr. Barry Eppley
Indianapolis, Indiana