

Background: Augmentation of the jaw angle region of the lower face can only be done on a permanent basis by an implant. It can be achieved with standard jaw angle implants or as part of a total custom jawline implant. But no matter how it is performed it involves the creation of a subperiosteal pocket over the jaw angle bone. In doing so elevation of the overlying masseter muscle is necessary.
The masseter muscle is typically described as part of a sling, known as the pterygomasseteric sling. This implies that there is a continuous connection between the inner lateral pterygoid muscle and that of the outer masseter muscle as it wraps around the inferior border of the jaw angle. In reality there is no muscular connection across the inferior border. Rather both muscles attach at the inferior border with a thin periosteal connection between the two which is attached to the bone.
Because of this thin connection along the inferior border, masseter muscle elevation must be done carefully to avoid detaching part or all of the muscular attachments. As a result the risk of partial masseteric muscle detachment and retraction can occur in any subperiosteal elevation for implant placement. This creates ‘implant reveal’ with lack of adequate tissue thickness over the most angular part of the implant. Should it occur a variety of treatment strategies can be employed included efforts at surgical muscle reattachment over the implant and camouflage efforts from injectable fillers and fat to cadaveric dermis coverage.
Case Study: This young male had jaw angle implants placed with some moderate masseteric muscle retraction on one side. This was most manifest to him by lack of a asymmetric jaw angle shape rather than a visible implant outline or a superior bulging muscle when chewing. He had prior efforts at soft tissue jaw angle augmentation with fat injections and the placement of a 2mm thick cadaveric dermal graft. (Alloderm) The fat did not persist at all and the Alloderm provided some improvement but further symmetry was desired.
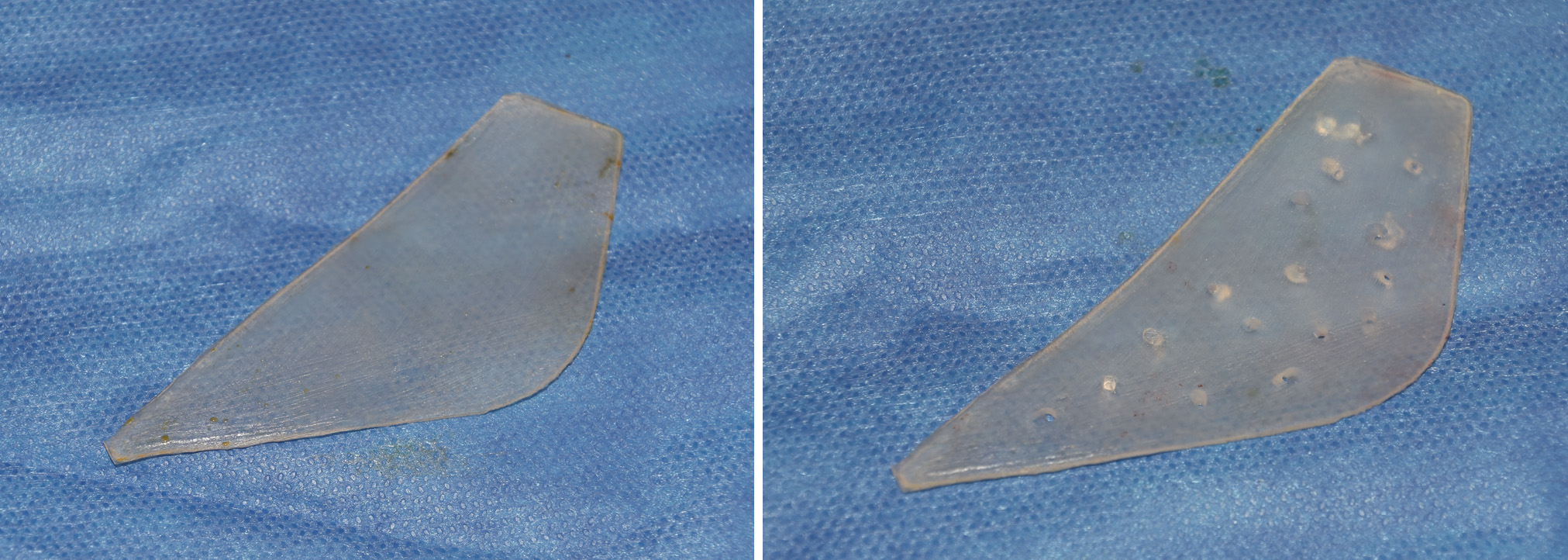
 To provide additional soft tissue jaw angle augmentation over the area of masseteric muscle retraction, a low durometer very soft solid silicone angle implant was designed. It matched the soft tissue defect and had an upper edge that was designed to go up over onto the muscle. It was 2.5mms at its thickest part near the angle. Multiple 2mm perfusion holes were placed throughout the implant prior to placement.
To provide additional soft tissue jaw angle augmentation over the area of masseteric muscle retraction, a low durometer very soft solid silicone angle implant was designed. It matched the soft tissue defect and had an upper edge that was designed to go up over onto the muscle. It was 2.5mms at its thickest part near the angle. Multiple 2mm perfusion holes were placed throughout the implant prior to placement.


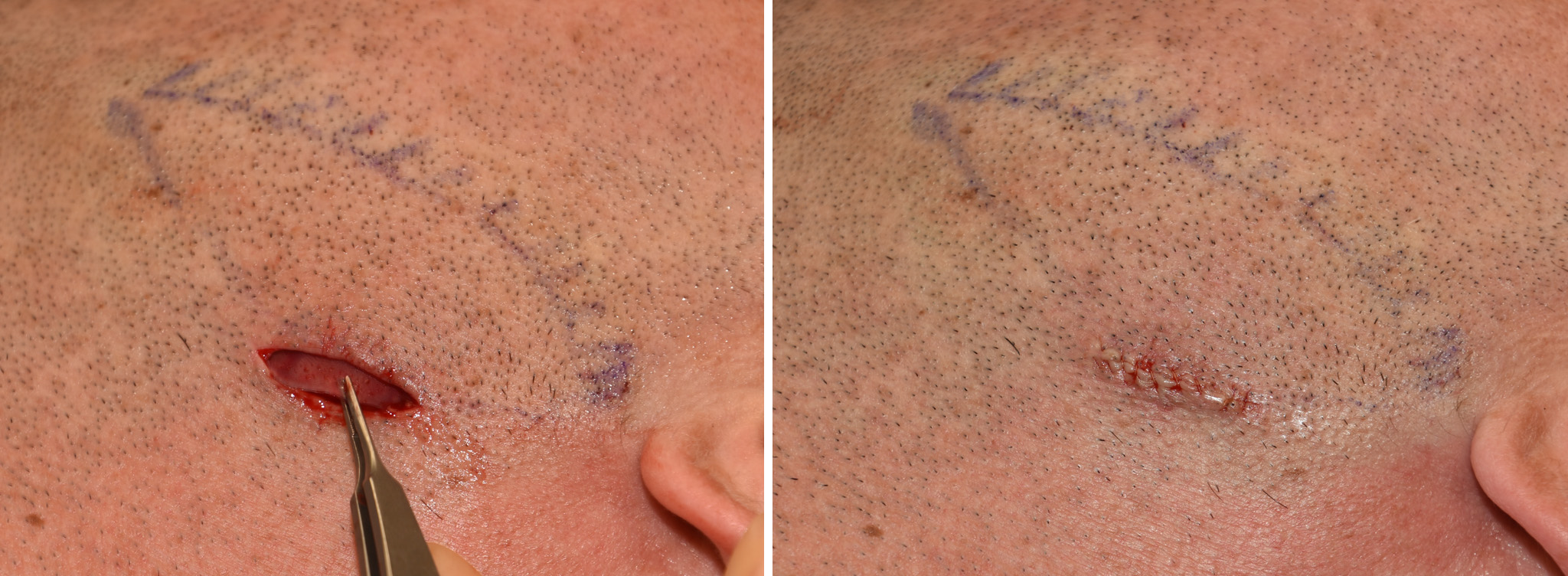 Through a 1 cm skin incision directly over the angle a subcutaneous pocket was developed going just beyond the skin markings. The previously placed Alldoerm graft could be identified. The implant was inserted making sure its thin upper perimeter edges were laying flat.
Through a 1 cm skin incision directly over the angle a subcutaneous pocket was developed going just beyond the skin markings. The previously placed Alldoerm graft could be identified. The implant was inserted making sure its thin upper perimeter edges were laying flat.
While masseteric muscle repositioning back over a jaw angle implant is the most biologic approach, it does not always work and patients may not desire a lather neck incision to do so. All of the camouflage soft tissue augmentation strategies have their merit and can be effective for some patients. But in refractory cases, a soft tissue silicone implant can provide a more assured augmentative outcome.
Case Highlights:
1) Masseteric muscle retraction is a potential aesthetic risk of any jaw angle implant procedure.
2) Surgically repositioning the muscle back over the implant involves an external scar and its effectiveness is not guaranteed.
3) A soft tissue jaw angle implant offers a direct approach to camouflaging implant reveal from masseteric muscular retraction.
Dr. Barry Eppley
Indianapolis, Indiana